
NL Journal of Dentistry and Oral Sciences
(ISSN: 3049-1053)
An Analytical and Statistical Study of Maxillary Sinus Pneumatization
Author(s) : Nesma Sherif Kassem, Jose Maria Suarez Quintanilla, Juan Antonio Suarez Quintanilla. DOI : 10.71168/NDO.02.02.112
Abstract
Background: A physiological process known as pneumatization of the maxillary sinus explains the sinus’s enlarging characteristics with aging. Objectives: The purpose of this study was to examine how age, sex, and race all of which are unmodified independent factors affect maxillary sinus pneumatization. Additionally, to determine which tooth on each side caused greater sinus pneumatization following extraction among Spanish and Egyptian patients. Materials and Methods: Two protocols were used using 440 panoramic x-rays to measurement digitally of the maxillary sinus pneumatization through recruited 220 Spanish and 220 Egyptian patients, both male and female, who were 20 years of age or older, with one or more maxillary posterior teeth extracted from the 1st premolar to the 3rd molar on each side with the contralateral side fully dentate. Results: Younger patients have a higher likelihood of sinus penetration with a root. The distance between the maxillary sinus and teeth is smaller in men than in women. No significant differences were observed between the right and left sides. In Spanish patients, the greatest pneumatization occurs after the extraction of the second molar, followed by the first molar. In Egyptian patients, the highest pneumatization is associated with the extraction of the second premolar, followed by the first molar. The distance to the maxillary sinus was statistically significant in both populations (P = 0.005, P = 0.012). Univariate analyses showed non-significant extraction effects, with varying effect sizes. The highest adjusted R² values were observed at the 1st molar in Egyptian patients and the 2nd molar in Spanish patients. Conclusion: In current, Maxillary sinus volume changes by age, as age increases the volume decreases. No significant difference as regard to gender with the tooth-sinus floor distance, but males show larger sinus than females. No significant difference is seen between right and left side in our sample. The large pneumatization occurs in cases of extraction of the 1st molar within the Spanish population, on other hand in Egyptian at level of the 2nd premolar. Keywords: Maxillary sinus, teeth extraction, pneumatization, Egypt, Spain.
Introduction
The maxillary sinus is the first paranasal sinus to develop, it is found at birth and expands by normal physiologic pneumatization during development, until the eruption of the upper third molar or the age of twenty years old [1,2]. Its normal extension is from the distal side of the canine to the posterior wall of the maxilla [3].
The function of maxillary sinus is not entirely known; however, it is known to lighten the weight of the skull, play a role in resonance and voice, and regulate the pressure of the nasal cavity. It was also suggested that it contributes in the defence of the nasal cavity due to the nitrogen monoxide it produces, that moreover humidifies and warms the inhaled air [4,5].
Dental procedures performed in the upper maxilla highly affect the maxillary sinus, as they are in close proximity, interventions including tooth extraction, implant placement, endodontic and orthodontic treatment if not done respecting the maxillary sinus extension can cause Schneiderian membrane perforation, displacement of the extracted tooth into the sinus or sinusitis [6,7,8].
Aside from the physiologic pneumatization of the maxillary sinus during development, scientists agreed that other pneumatization might take place after the extraction of one or more maxillary posterior teeth, causing decrease in the bone height and thus complicating the placement of dental implants [9,10], despite other theory states that the decrease in bone volume is due to the normal process of bone reabsorption after extraction and not to the sinus pneumatization [11,12].
Many studies investigated the relationship between the maxillary sinus and the underlying teeth, the majority agreed that maxillary molars are closer to the sinus than premolars [13,14], some concluded that the second molar is the nearest one to the sinus [13,14]. While other investigations deduced that the first molar is the closest maxillary molar to the sinus [15,16].
Other researchers focused more on that relationship and on the distance between the different roots of the maxillary molars and the sinus, a conclusion couldn’t be drawn, this could be explained by the variation of anatomy between populations [16,17].
This relation can be explored using different imaging techniques, but orthopantomographs are still the most frequent extraoral technique used in dentistry, as it provides the professional with information about a large number of anatomic structures, including the teeth, the maxillary sinus, both temporomandibular joints, all at a relatively low radiation dose and cost [18,19].
Although some studies stated that the exact relationship between maxillary posterior teeth and sinus cannot be interpreted through panoramic x-ray [20,21], Malina Altzinger et al [22] demonstrated that panoramic x-rays identified all findings like cone-beam computed tomography (CBCT) except the protrusion of the maxillary bone cyst into the sinus.
At the same time, other studies suggested that projection of the root into the sinus, darkening of the apical region involved in the sinus, interruption of the sinus floor are strong indicators of the actual protrusion of the root into the sinus [23,24].
The significance of implementing maxillary sinus pneumatization following tooth extractions is that we can assume that the loss of teeth causes maxillary sinus pneumatization, which in severe situations may result in a union between the sinus floor and the alveolar bone crest. According to some research comparing radiographs taken before and after extraction, maxillary sinus pneumatization could happen following the extraction of a posterior tooth [9]. Also, teeth extractions in the posterior maxilla may result in sinus pneumatization and crestal bone loss, with changes in the alveolar ridge and with or without socket preservation [25].
Therefore, the current study was done as primary objective maxillary sinus pneumatization degree according to various independent factors (protocol l) with specific goal identify the teeth that is provoking more pneumatization to the sinus after extraction among both sides (protocol 2).
Objectives
This study had various objectives, the primary one aimed to relate age, sex, and racial characteristics to the maxillary sinus pneumatization degree and was achieved by protocol 1.
While the secondary goal was to identify the tooth that is provoking more pneumatization to the sinus afterextraction in each population, protocol 2 was used.
Materials and Methods
Ethical approved
The study was approved by the Bioethics committee of the Faculty of Medicine and Dentistry, Santiago de Compostela University, Spain. After analyzing the reports from the corresponding working groups, which have assessed the methodological, ethical, and legal aspects of the research project, as well as the feasibility of the project in accordance with current legislation, The Committee of Ethics in Research of the USC AGREED to issue a FAVORABLE REPORT.
Project Title: Analytical and statistical study of the pneumatization of the maxillary sinus.
Study Design
A pre-experimental study (One-Shot Case Design), conducted at the department of oral surgery at Santiago de Compostela University in Spain, at geospatial coordinates (3.7492° W, 40.4637° N).
Sample Size
The necessary sample sizes for a study on maxillary sinus pneumatization after dental extractions were calculated using the G*Power program.
Egypt
For the extraction of the first molar, it was determined that 90 participants were needed.
The calculation was based on an effect size of 0.1778563, two predictors (gender and age), an alpha error of 0.05,
and a study power of 0.95.
Spain
For the extraction of the second molar, it was determined that 67 Spanish patients were needed.
The calculation was based on an effect size of 0.2437811, two predictors (gender and age), an alpha error of 0.05,
and a study power of 0.95.
In summary, the calculations helped determine the minimum number of participants needed for the study to have
sufficient statistical power in both populations.
Sample
In this study, a total of 440 panoramic radiographs were selected, 220 were selected from the archive of the Department of Oral Surgery in the faculty of Medicine and Dentistry in Santiago de Compostela University of Spanish subjects who had attended the department seeking dental treatment, and 220 panoramic radiographs from different radiographic centers in Alexandria, Egypt of Egyptian citizens.
Inclusion Criteria
- Radiographs of patients older than 20 years
- Radiographs clearly showing the roots of the maxillary posterior teeth, the floor of the maxillary sinus and the inferior orbital margin.
- Radiographs of patients, fully dentate or with one or more maxillary posterior teeth
Exclusion Criteria
- Radiographs of bad quality or showing
- Radiographs with any sinus pathology or of patients who had undergone bone regeneration procedure or implant placement in the posterior maxilla.
Image Acquisition and Measurements
All radiographs in Spain and Egypt were obtained by SIRONA Orthophos Plus DS (Sirona Dental Systems GmbH. Germany) for the caption of panoramic and cephalometric radiographs, normal panorama mode was used (p1) with voltage of 66 kVp, intensity of 16 mA, and exposure time of 14.1 s.
The measurements in both populations were done digitally using the SIDEXIS XG software provided by Sirona. Two protocols were used to assess the relationship between the maxillary sinus and the upper posterior teeth, and both of them were employed previously [26,9].
Protocol 1
It was used to achieve the primary goal of the study.
The outline of the maxillary sinus and the midline were traced digitally. To measure the distance between the root apex and the maxillary sinus floor two horizontal lines were traced, one at the end of the root apex and one marking the inferior border of the sinus floor in front of the root. These two horizontal lines were joined by a vertical line parallel to the midline. The distance between the maxillary sinus floor and the root apex was determined by measuring the vertical line, and classified into 3 classes:
Class 1: < 0 mm (excessive pneumatization).
Class 2: 0-3 mm (sinus approximation).
Class 3: > 3 mm (no sinus approximation).
Patients were also classified according to age into 3 groups:
Group 1: ≤ 30 years (young age).
Group 2: 31-50 years (middle age).
Group 3: ≥ 51 years (older age).
All teeth that were classified as Class I showed clearly an interruption in the sinus floor, darkening of the apical part of the root involved in the sinus or both findings [26] (Figure1).
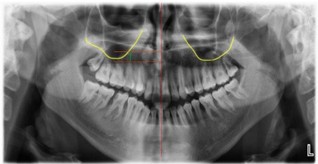
Figure 1: Measurement of the distance between the floor of the maxillary sinus and the apices of the posterior upper teeth.
Protocol 2
This protocol was applied on radiographs of patients who had one or more upper posterior teeth extracted on one side with the contralateral side fully dentate, in order to identify the maxillary posterior tooth that provoked the most pneumatization after being extracted.
Three reference horizontal lines were drawn, one joining the inferior border of the two orbits, and the other two marking the inferior border of the zygomatic arch on each side.
Two measurements were performed on each side:
- The distance between the interorbital line and the zygomatic
- The distance between the interorbital line and the inferior border of the sinus at the site of the studied
The null hypothesis is ISx/IZx=ISt/IZt where:
IS: vertical distance between the interorbital line and the most inferior point of the maxillary sinus at the area of the extracted tooth.
IZ: vertical distance between the interorbital line and the zygomatic arch line.
x: the side of extracted teeth. t: the side of existing teeth.
The sinus floor position is expressed as the following relation:
IS distance/ IZ distance
From the null hypothesis it’s concluded that the value ISx-(ISt*IZx/IZt) expresses the difference in the distance between the interorbital line and the sinus floor between both sides, if positive, it indicates that sinus floor was more inferior on the side of the extracted teeth [9] (Figure 2).
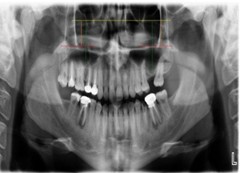
Figure 2: Reference lines used.
Results
A. Protocol 1
Spanish population
In the Spanish population age was seen to have a significant impact on the maxillary posterior teeth- sinus distance, as it affected that distance between all maxillary posterior teeth in female and male subjects except for the 2nd premolar in male subjects. It was found that Class I decreases by age in both sexes, and consequently the distance between teeth and sinus increases by age.
It was observed that sex significantly affected the distance between the upper wisdom tooth and the sinus in young age group (p˂0.001), while affecting the distance to the sinus in the case of the upper 2nd molar (p=0.045) in the middle age group, and the distance between all maxillary posterior molars and the sinus in the older age group (1st molar: p=0.015, 2nd molar: p=0.037, 3rd molar: p=0.006), with males showing higher percentage of Class I in all age groups than females. Right and left side didn’t show any significant differences in any tooth, neither in males nor in females (p>0.05).
Egyptian population
It was concluded that age significantly affected the distance between upper posterior teeth and the sinus, as was seen in the maxillary 2nd molar, first molar and 2nd premolar in males and females, in addition to the 1st premolar in females. It was observed that as age increases the percentage of finding a root penetrating the sinus (Class I) decreases, and that the distance between upper posterior teeth and the sinus tend to increase by age.
The results showed that sex affected the distance between the sinus and the second molar (p = 0.013), 1st molar (p = 0.007), and 2nd premolar (p = 0.039) in young age group (≤30 years), whereas the relation between the sinus and the 3rd molar was affected by sex in the middle age group (p = 0.038), (31-50 years). Additionally, males showed a higher percentage of class I than females in all age groups, indicating that males present larger maxillary sinus than females.
And finally, by comparing the distance between different teeth and the sinus floor, in the right and left side it was concluded that there is no statistical difference neither in males nor in females (p>0.05).
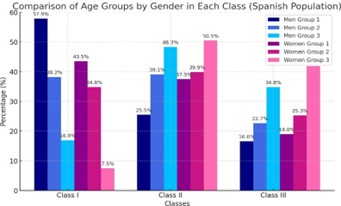
Table 1: Percentage of each class in different age groups of all teeth in Spanish population.
Ages Groups
Group 1: ≤ 30 years (young age).
Group 2: 31-50 years (middle age).
Group 3: ≥ 51 years (older age).
B. Protocol 2
Spanish population
In the Spanish population it was noticed that the amount of sinus pneumatization differed significantly after the extraction of different posterior teeth (p<0.001)
The major pneumatization occurred after the extraction of the maxillary 2nd molar with mean distance of (1.12 ± 0.48 mm) followed by the 1st molar (0.81 ± 0.41mm).
No difference was seen in the amount of maxillary sinus pneumatization after extraction of different teeth in males and females (p=0.968).
Egyptian population
As the Spanish population, in the Egyptian subjects it was viewed that pneumatization differs significantly according to the extracted tooth (p=0.002).
But in contrary to the Spanish study group, Egyptians showed greater pneumatization after the extraction of the maxillary 2nd premolar with a mean distance of 0.93±0.48 mm followed by the 1st molar (0.75±0.29 mm).
While no difference was found in the pneumatization after extraction between male and female subjects (p=1.000).
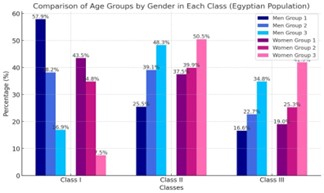
Table 2: Percentage of each class in different age groups of all teeth in Egyptian population.
Ages Groups
Group 1: ≤ 30 years (young age).
Group 2: 31-50 years (middle age).
Group 3: ≥ 51 years (older age).
Discussion
The size of maxillary sinus following tooth extraction was influenced by a number of causative factors; some of these factors may have contributed to the increase in size, while other factors did not show any discernible changes [27]. Furthermore, this heterogeneity has been documented with respect to a number of factors: non-modified factors included patient age and sex, while modified factors included tooth location, sinus floor configuration, sinus floor position with respect to the root apex, and the number of extracted teeth [28].
In order to compare the size of the maxillary sinus after the extraction of molar and premolar tooth on the left and right sides, the current study recruited 220 Egyptian patients and 220 Spanish patients, both male and female, who were 20 years of age or older.
In relation to the effect of gender on size of the maxillary sinus according to the position of tooth extraction from 1st premolar to the 3rd molar in both Egyptian and Spanish patients found that; there were no association between the patients’ gender and size of the maxillary sinus according to position of tooth extraction, according
to the study Maxillary Sinus Pneumatization Following Extractions in Riyadh, Saudi Arabia: A Cross-sectional Study by Alqahtani S., 2020 [14], the molar side groups, and gender groups did not exhibit any statistical significance and also by Siraj S. Najem 2021 [29] is showed that; statistically insignificant differences in maxillary sinus measurements between males and females. However, a 2019 study by Aktuna Belgin C [30] that used CBCT to evaluate the maxillary sinus volume in three dimensions across age and sex groups found that the males’ maxillary sinus volume was considerably larger than the females. Also, by Bornstein MM, 2019 is said that; males had significantly larger maxillary sinus volumes compared to females. This multiplicity contributed to the males tend to have a larger maxillary sinus than females can be utilized and implemented in forensic medicine to aid in gender determination. Furthermore, maxillary sinus assessment should be performed before placing temporary anchorage devices (TADs) in the maxilla to reduce the risk of sinus perforation. [31,32] in contrast to this view by Lim HC [33] is revealed that; women had more sinus expansion than men.
As regard to the effect of tooth position on maxillary sinus size, in current study in Egyptian patients found that; there was significant association between the means of maxillary sinus distance (mm) and the tooth type especially between the 1st premolar and the 2nd premolar, and between the 2nd premolar and the 2nd molar. On other hand in Spanish patients the significant association between the 1st premolar and the 2nd molar, and between the 2nd molar and 3rd molar. This may be due to Alveolar ridge remodeling, which involves an increase in the size of the maxillary sinus, may be triggered post-physiologically by the extraction of a posterior tooth in the maxilla. Clinically, ridge resorption in the coronal part of the extraction socket combined with maxillary sinus pneumatization (MSP) can reduce the amount of bone height accessible for future implant insertion. Disuse atrophy, which is characterized by a decrease in the mechanical strength of the bone tissue surrounding the extraction site, is sometimes assumed to include MSP maxillary sinus pneumatization [25,33].
Lim HC, et [33] found that; MSP was higher in the single tooth extraction (2.09±3.11 mm) than in the multiple tooth extraction (0.89±4.71 mm). First molars (1.90±4.02 mm), second premolars (0.78±3.07 mm), and first premolars (0.34±3.88 mm) were the tooth types with the largest extent of MSP, including second molars (2.25±4.39 mm). Out of all the causes for extraction, the extraction procedures conducted for endodontic issues resulted in the largest degree of sinus enlargement (2.28±2.37 mm). When compared to first premolars, second molars showed a statistically significant impact on MSP in the multiple mixed model (estimate: −2.35 mm, P=0.0177). Statistically significant differences were found between “unknown” and “periodontally compromised” reasons for extraction.
However, a higher level of MSP was noted in several extraction cases in the research by Sharan and Madjar and Jung et al [9,24]. (0.54±1.7 mm vs. 2.22±2.54 mm and 1.11±1.81 mm vs. 2.14±2.47 mm, respectively). According to the scientists, there may be a protective effect of the neighboring teeth’s roots against MSP. According to a different study by Hameed S. from 2019, only single-tooth extractions were included, and because of the nature of the studies (comparing non-grafted sockets to sockets with alveolar ridge preservation in the posterior maxilla), other studies did not examine the impact of single or multiple extractions [28]. This contributed to the greatest amount of MSP when the root of the maxillary tooth was surrounded by the upper curved border of the sinus floor (class V). In the study by Jung et al., the relationship between the sinus floor and the root apex had no significant impact on the extent of MSP. These discrepancies might be due to the difficulty in establishing the sinus floor on panoramic images, such as the difference in the position of the root apex on the buccal/palatal sides and furcal area. Jung YH, et al. [34] also may be due to an inflammatory response on the alveolar bone and sinus floor, given that, despite the small number of cases, the majority of teeth with SMT >10 mm had endodontic impairment. Endodontically compromised teeth exhibited the highest level of MSP among the reasons for extraction.
In confirmed to this hypothesis in a recent systematic review and meta-analysis, 1,550 maxillary sinuses related to peri-apical lesions were analyzed, demonstrating that the presence of periapical lesions was associated with up to a 2.43-fold greater risk of SMT >2 mm [35]. A study showed that a periapical lesion next to the maxillary sinus might be an origin of the spread of odontogenic bacteria, provoking SMT [36]. In particular, when the alveolar bone apical to the root apex is thin, extraction of a tooth with an apical lesion and severe SMT may exacerbate the resorption of the adjacent bone concomitantly with bundle bone resorption. In contrast, in the study by Hammed et al., SMT did not affect MSP, but they did not present the extent of SMT or the reason for extraction [27].
It is noteworthy that there is a statistically significant correlation between MSP and the extraction of the second molar in the multiple mixed models. This region is close to the sinus floor and has low bone density. These features may enhance MSP in the second molar area compared to other sites. Because of its most distal location, the second molar area could be the most challenging to reach and see. Consequently, it could be advantageous to devise a strategy to offset MSP in this region prior to extraction. Alveolar ridge preservation (ARP) could be one way to achieve this goal.
There are a few published studies that support ARP in the posterior maxilla [37]. The sinus floor in the sockets with and without ARP changed by −0.30±0.10 mm and −1.30±0.27 mm, respectively, according to the study by Levi et al. With a sinus floor level shift of -1.16 mm in sockets without ARP and -0.14 mm in sockets with ARP, the study by Rasperini G et al. also supported ARP. Because of ARP’s beneficial effects, implant surgery for the second molar region may become more feasible [38].
The limitations of this study include a lack of pre-extraction records such as time elapsed since the extraction and radiographs, in addition to the amount of bone loss during the extraction.
Conclusion
The current study’s findings shown that the maxillary sinus volume varies with age, decreasing with increasing age. In Egyptian and Spanish populations, males had larger sinuses than females. The extraction of the maxillary second molar followed by the first molar in the Spanish population exhibited larger pneumatization, whereas the extraction of the second premolar followed by the first molar in the Egyptian population demonstrated that sinus pneumatization following extraction may differ among populations. In our sample, there was no discernible difference between the right and left sides.
References
1. Thomas von Arx, Scott Lozanoff. Maxillary Sinus. In: Thomas von Arx, Scott Lozanoff, editors. Clinical Oral Anatomy A Comprehensive Review for Dental Practitioners and Researchers. Switzerland: Springer Nature; 2017. p. 163-97.
2. Jun BC, Song SW, Park CS, Lee DH, Cho KJ, Cho JH. The analysis of maxillary sinus aeration according to aging process; volume assessment by 3-dimensional reconstruction by highresolutional CT scanning. Otolaryngol Head Neck Surg. 2005; 132(3):429–34.
3. Stuart C White, Michael J Pharoah. Normal Radiographic Anatomy. In: Stuart C White, Michael J Pharoah, editors. Oral Radiology Principles and interpretation. 6th ed. US: Mosby Elsevier; 2009. p.152-74.
4. Jankowski R, Nguyen DT, Poussel M, Chenuel B, Gallet P, Rumeau C. Sinusology. Eur Ann Otorhinolaryngol Head Neck Dis. 2016 Sep; 133(4):263–8.
5. Sieron HL, Sommer F, Hoffmann TK, Grossi A-S, Scheithauer MO, Stupp F, et al. [Function and physiology of the maxillary sinus]. HNO. 2020; 68(8):566–72.
6. Seigneur M, Cloitre A, Malard O, Lesclous P. Teeth roots displacement in the maxillary sinus: characteristics and management. Oral Med. Oral Surg. 2020; 26(3):34.
7. Sun W, Xia K, Huang X, Cen X, Liu Q, Liu J. Knowledge of orthodontic tooth movement through the maxillary sinus: a systematic review. BMC Oral Health. 2018; 18(1):91-100.
8. Brooks JK, Kleinman JW. Retrieval of extensive gutta-percha extruded into the maxillary sinus: use of 3-dimensional cone beam computed tomography. J Endod. 2013; 39(9):1189-93.
9. Sharan A, Madjar D. Maxillary sinus pneumatization following extractions: a radiographic study. Int J Oral Maxillofac Implants. 2008; 23(1):48-56.
10. Alqahtani S, Alsheraimi A, Alshareef A, Alsaban R, Alqahtani A, Almgran M, et al. Maxillary Sinus Pneumatization Following Extractions in Riyadh, Saudi Arabia: A Cross-sectional Study. Cureus. 2020; 12(1):6611.
11. Schriber M, Bornstein MM, Suter VGA. Is the pneumatisation of the maxillary sinus following tooth loss a reality? A retrospective analysis using cone beam computed tomography and a customised software program. Clin Oral Investig. 2019; 23(3): 1349-58.
12. Chen YW, Finkelman M, Papaspirisdakos P, César-Neto JB, Weber HP, de Souza AB. Comparative analysis of dimensional alterations following extraction of maxillary molars using three-dimensional images’ superimposition: a CBCT study. Odontology. 2021; 109(2): 514-23. 478
13. Makris LML, Devito KL, D’Addazio PSS, Lima CO, Campos CN. Relationship of maxillary posterior roots to the maxillary sinus and cortical bone: a cone beam computed tomographic study. Gen Dent. 2020; 68(2):e1-e4.
14. Kang SH, Kim BS, Kim Y. Proximity of Posterior Teeth to the Maxillary Sinus and Buccal Bone Thickness: A Biometric Assessment Using Cone-beam Computed Tomography. J Endod. 2015; 41(11):1839-46.
15. Lupoi D, Dragomir M, Coada G, Sanda A, Budu V. CT scan evaluation of the distance between maxillary sinus floor and maxillary teeth apices. Rom. J. Rhinol. 2021; 11(41):18-23.
16. Fry RR, Patidar DC, Goyal S, Malhotra A. Proximity of maxillary posterior teeth roots to maxillary sinus and adjacent structures using Denta scan® . Indian J Dent. 2016; 7(3):126-30.
17. Jang JK, Kwak SW, Ha JH, Kim HC. Anatomical relationship of maxillary posterior teeth with the sinus floor and buccal cortex. J Oral Rehabil. 2017; 44(8):617-25.
18. Różyło-Kalinowska I. Panoramic radiography in dentistry. Clin Dent Rev. 2021; 5(1): 26.
19. Sun W, Xia K, Tang L, Liu C, Zou L, Liu J. Accuracy of panoramic radiography in diagnosing maxillary sinus-root relationship: A systematic review and meta-analysis. Angle Orthod. 2018; 88(6): 819–29
20. Shahbazian M, Vandewoude C, Wyatt J, Jacobs R. Comparative assessment of panoramic radiography and CBCT imaging for radiodiagnostics in the posterior maxilla. Clin Oral Investig. 2014; 18(1):293-300.
21. Terlemez A, Tassoker M, Kizilcakaya M, Gulec M. Comparison of cone-beam computed tomography and panoramic radiography in the evaluation of maxillary sinus pathology related to maxillary posterior teeth: Do apical lesions increase the risk of maxillary sinus pathology?. Imaging Sci Dent. 2019; 49(2):115-22.
22. Malina-Altzinger J, Damerau G, Grätz KW, Stadlinger PD. Evaluation of the maxillary sinus in panoramic radiography-a comparative study. Int J Implant Dent. 2015; 1(1):17.
23. Themkumkwun S, Kitisubkanchana J, Waikakul A, Boonsiriseth K. Maxillary molar root protrusion into the maxillary sinus: a comparison of cone beam computed tomography and panoramic findings. Int J Oral Maxillofac Surg. 2019; 48(12):1570-6.
24. Jung YH, Cho BH, Hwang JJ. Comparison of panoramic radiography and cone-beam computed tomography for assessing radiographic signs indicating root protrusion into the maxillary sinus. Imaging Sci Dent. 2020; 50(4): 309-18.
25. Levi I, Halperin-Sternfeld M, Horwitz J, Zigdon-Giladi H, Machtei EE. Dimensional changes of the maxillary sinus following tooth extraction in the posterior maxilla with and without socket preservation. Clin Implant Dent Relat Res. 2017; 19:952–958. https://doi:10.1111/cid.12521
26. Elsayed SA, Alolayan AB, Alahmadi A, Kassim S. Revisited maxillary sinus pneumatization narrative of observation in Al-Madinah Al-Munawwarah, Saudi Arabia: A retrospective cross- sectional study. Saudi Dent J. 2019;31(2):212-218. doi:10.1016/j.sdentj.2018.11.002
27. Hameed S, Bakhshalian N, Alwazan E, Wallace SS, Zadeh HH. Maxillary sinus floor and alveolar crest alterations following extraction of single maxillary molars: a retrospective CBCT analysis. Int J Periodontics Restorative Dent. 2019; 39:545 551. https://:doi:10.11607/prd.3865
28. Cha JK, Song YW, Park SH, Jung RE, Jung UW, Thoma DS. Alveolar ridge preservation in the posterior maxilla reduces vertical dimensional change: a randomized controlled clinical trial. Clin Oral Implants Res. 2019; 30:515–523.https://:doi:10.1111/clr.1343
29. Siraj S. Najem email 1; Wael M. Safwat2; Rania A. ELAziz3; Yousria S. Gaweesh. maxillary sinus assessment for gender and age determination using cone beam computed tomography in an egyptian sample. 2021; 10(2):63-69. https://: DOI: 10.21608/ADJALEXU.2020.88457
30. Aktuna Belgin C, Colak M, Adiguzel O, Akkus Z, Orhan K. Three-dimensional evaluation of maxillary sinus volume in different age and sex groups using CBCT. Eur Arch Otorhinolaryngol. 2019; 276(5):1493-1499. https://:doi:10.1007/s00405-019-05383-y
31. Asantogrol F, Etoz M, Topsakal KG, Can FE. Evaluation of the maxillary sinus volume and dimensions in different skeletal classes using cone beam computed tomography. Ann Med Res. 2021; 28:709–15.
32. Alqahtani H, Basuhail S, Alsulaimani F, Zawawi KH, Barayan M, Al Turki G, Abbassy MA. The Relationship between Maxillary Sinus Volume and Different Cephalometric Characteristics in Orthodontics. Contemp Clin Dent. 2023; 14(3): 191-200. https://doi:10.4103/ccd.ccd_548_22.
33. Lim HC, Kim S, Kim DH, Herr Y, Chung JH, Shin SI. Factors affecting maxillary sinus pneumatization following posterior maxillary tooth extraction. J Periodontal Implant Sci. 2021; 51(4):285-295. https://doi:10.5051/jpis.2007220361
34. Jung YH, Nah KS, Cho BH. Maxillary sinus pneumatization after maxillary molar extraction assessed with cone beam computed tomography. Korean J Oral Maxillofac Radiol. 2019; 39:109– 113.
35. Peñarrocha-Oltra S, Soto-Peñaloza D, Bagán-Debón L, Bagan JV, Peñarrocha-Oltra D. Association between maxillary sinus pathology and odontogenic lesions in patients evaluated by cone beam computed tomography. A systematic review and meta-analysis. Med Oral Patol Oral Cir Bucal. 2020; 25:34–48. https://doi:10.4317/medoral.23172.
36. Huang YT, Hu SW, Huang JY, Chang YC. Assessment of relationship between maxillary sinus membrane thickening and the adjacent teeth health by cone-beam computed tomography. J Dent Sci. 2021; 16:275–279. https://doi:10.1016/j. jds.2020.05.002.
37. Almasoud NN, Tanneru N, Marei HF. Alveolar bone density and its clinical implication in the placement of dental implants and orthodontic mini-implants. Saudi Med J. 2016; 37:684–689. https://doi:10.15537/smj.2016.6.14274.
38. Rasperini G, Canullo L, Dellavia C, Pellegrini G, Simion M. Socket grafting in the posterior maxilla reduces the need for sinus augmentation. Int J Periodontics Restorative Dent. 2020; 30:265– 273.
This article licensed under the Creative Commons Attribution 4.0 International License CC-BY 4.0., which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are properly credited.