
NL Journal of Dentistry and Oral Sciences
(ISSN: 3049-1053)
Epidemiology of Oral Cancers among Sudanese population at Khartoum Dental Teaching Hospital, Khartoum, Sudan
Author(s) : Eman Hafiz Sidahmed Suliman, Khidir Faisal Abubaker Mahmoud. DOI : 10.71168/NDO.02.02.110
Abstract
Background: Oral cancer (OC) is becoming more common everywhere, making it a significant contributor to the overall burden of cancers. With 920 instances annually, OC is the sixth most prevalent cancer type in Sudan and accounts for 9% of all cases recorded each year in Africa. This study’s goals were to examine the epidemiology of oral cancer and detail any instances that were reported to Khartoum Teaching Dental Hospital between 2014 and 2015. Material and Methods: This is descriptive cross-sectional hospital-based study with two components: retrospective and exist survey. All files of the patients which were diagnosed as oral cancer and have been operated were selected. Record-based data collected using a form and exist survey data collected using a questionnaire. Data entered and analyzed using the SPSS. Results: A total of 224 patients were studied. Their age ranged from 4 to 87 years and) 33% (of them were 61 and above years. Around two thirds (59.8%) were male. And about one third (28.6 %) of the respondents were from Khartoum state. Squamous cell carcinoma (SCC) represents 60.8% of cases. A total of 125 cases (66.1%) showed good prognosis. Conclusion: Male patients made up more of the oral cancer patient population than female patients, and the bulk of cases originated in Khartoum state. Oral cancer patients were typically 61 years of age or older. Keywords: Squamous cell carcinoma, Human Papilloma virus, Precancerous, Radiation therapy.
Introduction
Oral cancer has been recognized as a huge threat to public health because of its high morbidity and mortality. It is estimated that each year there are over 484,000 people diagnosed with oral cancer in the world and approximately 261,000 people die of this disease [1]. In China, over 11,900 cases of oral cancers are diagnosed each year and approximately 5,000 patients die of the disease [1]. A number of factors are associated with the increase of risks of oral cancer. The risk factors include age, tobacco and alcohol consumption, human papilloma virus infection, and race, etc [2,3,4]. Primary treatments of oral cancer include surgery, radiation and chemotherapy [3,5,6]. These treatments can be employed alone or in combination depending on the clinical stage and histology of oral cancer.
Beside primary treatments, oral cancer patients may require additional care to ameliorate the side effects of treatment, such as oral pain due to the tumor or oral mucositis, weight loss, fatigue, nausea, vomiting, and altered salivary gland function [7,8]. Although many studies were carried out in the area of oral cancer, still there is a gap in our knowledge. The distribution of cases according to age, gender, residence and the type of oral cancer need to be explored more. The direct cost related to oral cancer need to be more explored also.
Oral Cancer Overview
Of the more than 34,000 new patients diagnosed with oral cancer in the United States annually, only half live past the five-year survival milestone [9].
Approximately 6,900 Americans die annually and for those who do survive, many are severely disfigured and suffer compromised lives [9].
People who use tobacco products tend to have a higher risk for oral cancer, and those who use tobacco products and consume excessive alcohol have an especially high risk [10].
Of those diagnosed, 25% have no risk factors [11,12] Risk increases for tobacco users, excessive alcohol consumption, overexposure to sunlight and poor nutrition [13]. Oral cancer has also been linked with human papilloma viruses, more commonly called HPVs [13].
Oral cancer is twice as common in men as in women [14]. However, women are among the fastest-growing segments of those being diagnosed, as well as non-smokers and people under 40-years-old [15].
The average age of those diagnosed with oral cancer is 62 years old, but about one-third of those diagnosed are under 55- years-old [14].
The most prevalent oral cancer sites are the tongue, floor of the mouth and the soft palate, but it also may be found on the lips, cheeks or gums.
Early Detection
If oral cancer is detected in the precancerous stage, it can be prevented. Other benefits of early detection include: Treatment may be less invasive, treatment costs are lower and recovery time is minimized [16].
If caught early enough, the five-year survival rate jumps to 82.7% for localized oral cancer [16].
Results
The distribution of the patients according to the age is shown in table 1. The age of the patients ranged from four years to 87 years in which (33%) were 61 and above years. The distribution of patients according to gender is shown in figure 1 Male patients were (59.8%) while (40.2) were females.
About one third (28.6 %) of the respondents were from Khartoum state followed by (16.5%) from Kurdofan states. Table 2.
The distribution of the patients according to marital status is shown in figure 2. About (76.8%) were married while (17%) were single and only (1.8%) were children. occupation and the result is shown in Table 3. Workers and housewives represent (27.7%) respectively, while (19.6%) were farmers.
The distribution of study sample according to type of cancer is shown in table 4. Squamous cell carcinoma (SCC) represents more than half of the study sample (60.8%). Patients who had complete recovery were 61 patients (32.2%), while patients whom prognosis were better were 125 patients (66.1%). however, only two patients passed away Figure 3.
| Age | Frequency | percent (%) |
| <10 | 6 | 2.7 |
| 11-20 | 15 | 6.7 |
| 21-30 | 25 | 11.2 |
| 31-40 | 17 | 7.6 |
| 41-50 | 39 | 17.4 |
| 51-60 | 48 | 21.4 |
| 60 and above | 74 | 33.0 |
| Total | 224 | 100.0 |
Table 1: Distribution of study sample according to (Age) in KTDH 2014-2015
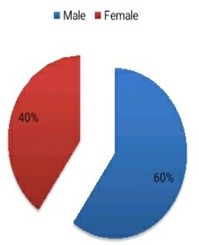
Figure 1: Distribution of study sample cording to Gender in KTDH 2014-2015
| Frequency | Percent (%) | |
| Al Khartoum state | 64 | 28.6 |
| Al Gazeera state | 29 | 12.9 |
| Kurdofan states | 37 | 16.5 |
| White Nile state | 25 | 11.2 |
| Northern state | 20 | 8.9 |
| Red sea state | 13 | 5.8 |
| Blue Nile state | 5 | 2.2 |
| Dar foor states | 13 | 5.8 |
| River Nile state | 10 | 4.5 |
| Sennar state | 5 | 2.2 |
| Others | 3 | 1.3 |
| Total | 224 | 100.0 |
Table 2: Distribution of study sample according to (State) in KTDH 2014-2015
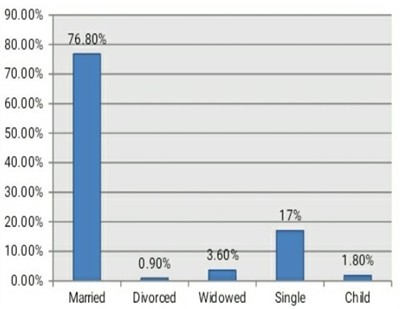
Figure 2: Distribution of study sample cording to marital status in KTDH 2014-2015
| Occupation | Frequency | percent (%) |
| Farmer | 44 | 19.6 |
| Worker | 62 | 27.7 |
| House wife | 62 | 27.7 |
| Student | 25 | 11.2 |
| Retired | 14 | 6.3 |
| Employee | 10 | 4.5 |
| Teacher | 3 | 1.3 |
| Child | 4 | 1.8 |
| Total | 224 | 100.0 |
Table 3: Distribution of study sample cording to (Occupation) in KTDH 2014-2015
| Frequency | percent (%) | |
| S.C.C | 136 | 60.8 |
| Ameloblastic carcinoma | 29 | 13.1 |
| Myoepithelium carcinoma | 13 | 6.1 |
| Mucoepidermoid carcinoma | 10 | 4.4 |
| Adenocarcinoma | 10 | 4.4 |
| Verrocus carcinoma | 8 | 3.5 |
| Ca. tongue | 6 | 2.6 |
| Basal cell carcinoma | 5 | 2.1 |
| Non-Hodgkin’s lymphoma | 4 | 1.7 |
| Papillary carcinoma | 2 | 0.9 |
| Burkitt’s lymphoma | 1 | 0.4 |
| Total | 224 | 100.0 |
Table 4: Distribution of study sample cording to (Type of cancer) in KTDH 2014-2015
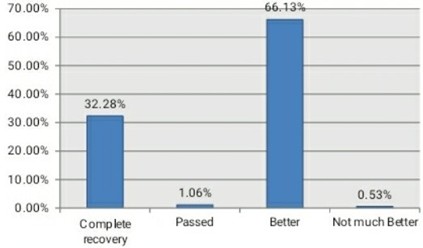
Figure 3: Distribution of study sample cording to Prognosis in KTDH 2014-2015
Discussion
In this study the epidemiology of oral cancer was described in terms of age, gender, residence and types cancer. About (33%) of the respondents who had oral cancer ware 61 and above years old in which (59.8%) were males and (40.2%) were females. A study conducted by (Esraa Mosalleum 2014) stated that the peak age of oral and -lip cancers were 75 years for females and 65-69 years for males. The prevalence of OSCC above the age of 50 years was 79% and 76% for males and females respectively [17].
SCC represent the majority of oral cancer types, more than half of the study sample (60.8%). A study conducted by (Esraa Mosalleum 2014) stated that the most common type of malignancy reported was SCC which accounted for (66.5%) in Sudan [17].
In present study Khartoum state represent about (28.6%) which is the highest rate of distribution of oral cancer patients studied in this research, kourdofan state was (16.5%)while Aljazeera state about ( 12.9%),in another study conducted found that Analysis of the geographical distribution of the cases recorded in KDTH revealed that only 5% of the cases originated from the South, compared to 28% from Khartoum state, 15% from Gezira state, 21% from the Eastern states collectively and another research conducted stated that northern Sudanese suffer from a high rate of SCC while southern Sudanese endure a higher rate of odontogenic and salivary gland neoplasm (Idris et al, 1995) [18].
Prognosis of registered cases
Regarding the prognosis of registered cases which included in this study, were 61 patients (32.2%) had complete recovery, while patients whom prognosis were better were 125 patients (66.1%). however only two patients passed away.
Conclusion
The study revealed that:
The majority of patients with oral cancer were 61 and above years old.
Male patients were more than female patients,
Majority of cases came from Khartoum state represent.
References
1. Ferlay J, Bray F, Pisani P, Parkin DM. IARC Cancer Base No. 5. Version 2.0. Lyon: IARC Press; 2004. GLOBOCAN 2002: Cancer incidence, mortality and prevalence worldwide.
2. Laronde DM, Hislop TG, Elwood JM, Rosin MP. Oral cancer: just the facts. J Can Dent Assoc. 2008; 74:269–72.
3. Kademani D. Oral cancer. Mayo Clin Proc. 2007; 82:878–87. doi: 10.4065/82.7.878.
4. Schwartz SM, Daling JR, Doody DR, Wipf GC, Carter JJ, Madeleine MM, Mao EJ, Fitzgibbons ED, Huang S, Beckmann AM, McDougall JK, Galloway DA. Oral cancer risk in relation to sexual history and evidence of human papillomavirus infection. J Natl Cancer Inst. 1998; 90:1626–36. doi: 10.1093/jnci/90.21.1626.
5. Hollows P, McAndrew PG, Perini MG. Delays in the referral and treatment of oral squamous cell carcinoma. Br Dent J. 2000; 188:262–65. doi: 10.1038/sj.bdj.4800449a.
6. The Early Detection of Oral Cancer Working Group. Guideline for the early detection of oral cancer in British Columbia 2008. BC Oral Cancer Prevention Program of the BC Cancer Agency. 2008. http://www.cdsbc.org/pdf/OC_Guideline_Final_2008.pdf
7. Barker GJ, Epstein JB, Williams KB, Gorsky M, Raber-Durlacher JE. Current practice and knowledge of oral care for cancer patients: a survey of supportive healthcare providers. Support Care Cancer. 2005; 13:32–41. doi: 10.1007/s00520-0040691-5.
8. Epstein JB, Parker IR, Epstein MS, Stevenson-Moore P. Cancer-related oral health care services and resources: a survey of oral and dental care in Canadian cancer centers. J Can Dent Assoc. 2004; 70:302–4.
9. Cancer Facts & Figures 2011.” (2011). American Cancer Society. http://www.cancer.org/acs/groups/content/@epidemiologysurveilance/documents/document/acspc-029771.pdf
10. Oral Cancer Foundation, http://oralcancerfoundation. org/facts/alcohol_tobacco.htm, accessed April 2011.
11. Schantz SP, Yu GP. Head and neck cancer incidence trends in young Americans, 1973-1997, with a special analysis for tongue cancer. Arch Otolaryngol Head Neck Surg. Mar 2002;128(3):268-274.
12. Lingen M, Sturgis EM, Kies MS. Squamous cell carcinoma of the head and neck in nonsmokers: clinical and biologic characteristics and implications for management. Curr Opin Oncol. May 2001;13(3):176-182
13. American Cancer Society, http://www.cancer.org/Cancer/ OralCavityandOropharyngealCancer/DetailedGuide/oral cavity-and-oropharyngeal-cancer-risk-factors, accessed July 2011.
14. American Cancer Society, http://www.cancer.org/Cancer/ OralCavity andOropharyngealCancer/DetailedGuide/oral cavity-and-oropharyngeal-cancer-key-statistics, accessed July 2011.
15. The Oral Cancer Foundation, http://oralcancer foundation.org/facts/index.htm, accessed June 2011.
16. National Cancer Institute, SEER Oral Cancer Survival Rates, 1999-2005.
17. Esraa Mosalleum, Epidemiology of Oral Malignancies in the Sudan (2004-2008) University of the Western Cape, Cape Town, South Africa, 2014.
18. Idris, A.M., Ahmed, H.M., Mukhtar, B., I., Gadir, A., F., EL-beshir, E., I., 1995. Descriptive epidemiology of oral neoplasms in Sudan 1970-1985 and the role of toombak. Int J Cancer; 61(2): 155-8.
This article licensed under the Creative Commons Attribution 4.0 International License CC-BY 4.0., which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are properly credited.