
NL Journal of Dentistry and Oral Sciences
(ISSN: 3049-1053)
Fan Shaped Expander for Narrow Arch- A Case Series
Author(s) : Varun Goyal, Ravi, Sachin Philip, Raj Kumar Singh, Gurkeerat Singh, Sridhar Kannan, Triparna Kapoor, Sushma Chaurasia. DOI : 10.71168/NDO.01.01.111
Abstract
Transverse discrepancy can lead to various malocclusions so it should be treated as early as possible. Arch expansion is novel technique and to correct transverse discrepancy RME is more advantageous than SME as it brings skeletal and dental changes more rapidly. In some cases of narrow ‘V’ constricted arches use of standard RME can distrupt normal molar relations in posterior region so fan shaped RME is of greater significance. This case series shows changes produced by fan shaped expander and increase in intercanine width with minimal posterior changes.
Introduction
There are very limited published case reports showing clinical efficacy of fan shaped expander so this case series will be helpful in understanding the effects clinically and treatment outcome. Transverse deficiency of maxillary arch can lead to deficient development of maxillary bone and adjacent structures. It can be due to abnormal nasal breathing, any trauma and congenital abnormalities like cleft lip and palate and developmental. Transverse deficiency can lead to crowding, Class II malocclusion, scissor bite and posterior crossbite [1]. Posterior crossbite can cause alteration in skeletal growth, myofunctional alteration, asymmetrical positioning of condyle and temporomandibular disorder [2-4]. Arch expansion is a method to correct transverse deficiency and space gaining [5]. One of the main objective of arch expansion is to coordinate maxillary and mandibular denture base. The technique to correct transverse deficiency is skeletal, dental and surgical [6]. Based on number of activations maxillary expansion is divided into rapid maxillary expansion (RME) and slow maxillary expansion (SME). In 1860, Emerson C. Angell first used rapid maxillary expansion device to increase transverse width in maxillary arch [7,8]. RME causes more rapid maxillary expansion and activation of RME is described as 0.5–1 mm/day [9]. There are various types of removable and fixed RME appliances such as Issacson and HYRAX (Tooth borne) and Derichsweiler and Hass (Tooth-Tissue borne). Ordinary RME (Figure 1a) expansion screw exerts parallel fore to maxillary complex and alveolar bone. In some cases, occlusion in molar region is normal but crossbite is present in anterior canine and bicuspid region so in such cases expansion force should be in such a way that it does not cause buccal tipping of the teeth with minimal expansion in posterior region.
To solve this problem a fan shaped expander (Figure 1b) has been designed by Schellino and Modica which produces differential expansion [10]. It has an expansion screw named “ragno” and it allows opening of suture in ‘V’ pattern. Since there are very limited literature and published case reports on Fan-shaped RME, this article would be enlightening.
 Figure 1: RME a) Standard RME b) Fan shaped RME
Figure 1: RME a) Standard RME b) Fan shaped RME
Rationale for Fan-shaped RME
- Narrow constricted maxilla requiring a selective anterior expansion such as in cases of cleft palate patients.
- Upper arch with no posterior crossbite and the molar width is normal.
- Upper arch which requires more inter canine width expansion than inter molar width.
Case I Diagnosis
A female patient aged 13 years reported to Department of Orthodontics and Dentofacial Orthopaedics with chief complaint of irregularly placed upper front teeth. She had a history of trauma wrt deciduous upper right central incisor at the age of 2 years. Extraoral examination showed a symmetrical face, convex profile, obtuse nasolabial angle, average growth pattern and competent lips (Figure 2). Smile analysis found a consonant smile arc. Upper and lower dental midline was matching. Intraorally, she had a class I molar relation on the left side and right side with overjet of 2 mm and overbite of 3 mm. The lower anterior teeth had a mild amount of crowding and retained upper right and left deciduous canine was present. She had a narrow V-shaped maxillary arch (Figure 2)
 Figure 2: Pre-treatment extraoral and intraoral photographs
Figure 2: Pre-treatment extraoral and intraoral photographs
Cephalometric analysis showed a Class I skeletal jaw base (ANB angle = 3°), average mandibular plane angle (FMA = 27o). On dental analysis, she had upright upper and lower incisors (U1-NA = 20/3° and L1-NB = 23/4°). The panoramic radiograph showed impacted upper left and right permanent canine Sector I according to modified Erickson and kurol and no mandibular asymmetry with normal shape and size of the condyles with apparently equal ramal and body length bilaterally. No pathological radiopacity/radiolucency seen (Figure 3).
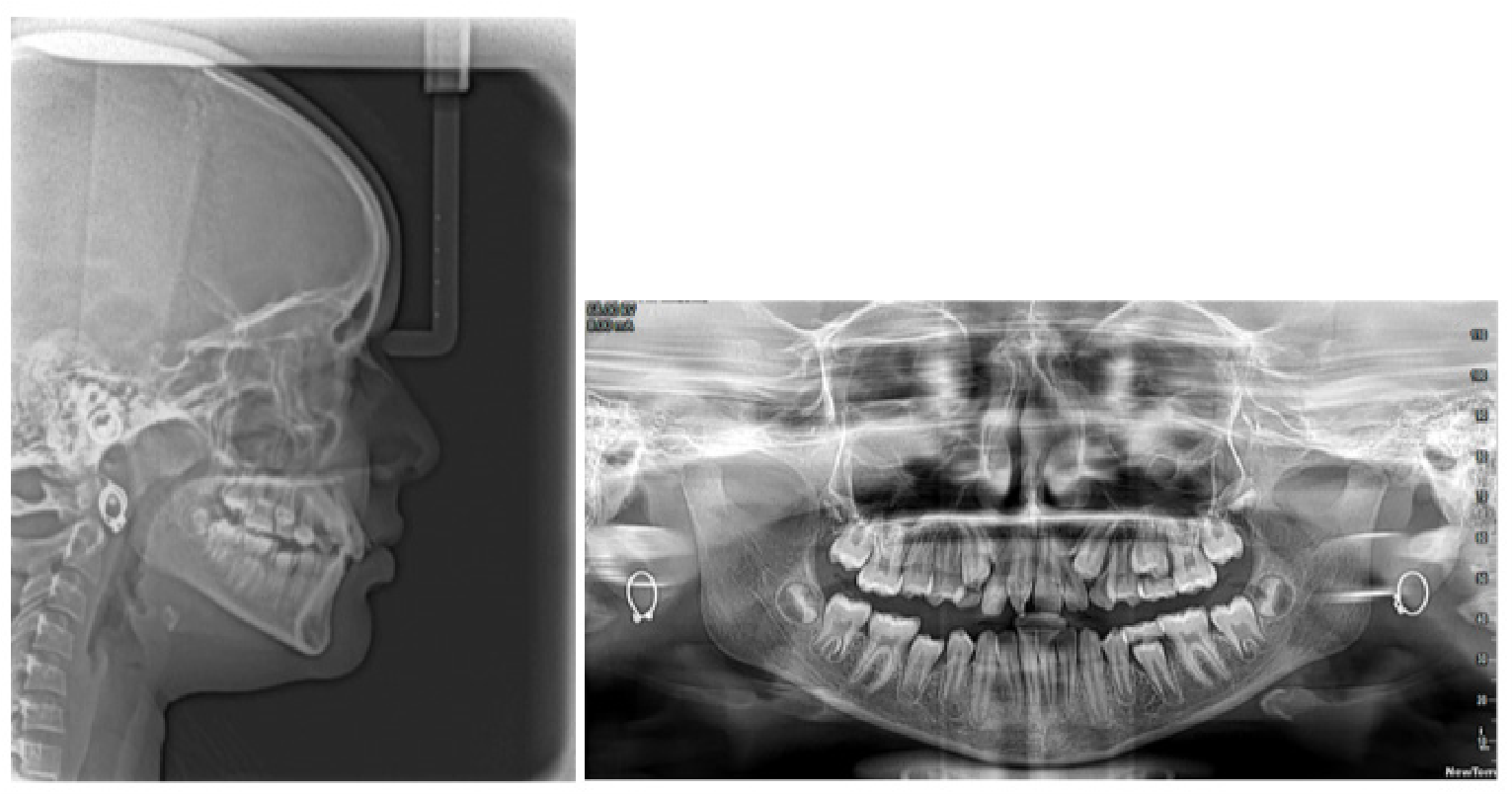 Figure 3: Pre-treatment lateral cephalogram and panaromic radiograph
Figure 3: Pre-treatment lateral cephalogram and panaromic radiograph
Occlusal radiograph showed stage C of mid-palatal suture ossification (Figure 4). Ashley howe analysis showed premolar basal arch width (PMBAW) is more than Premolar diameter (PMD) so it was an indication that basal arch is sufficient to allow expansion.
 Figure 4: Pre-treatment occlusal radiograph
Figure 4: Pre-treatment occlusal radiograph
The main objective of orthodontic treatment was expansion of constricted maxillary arch with sequential eruption of permanent teeth and to correct rotation, crowding and achievement of Class I molar and Class I canine relationship on both the sides achieving harmonious soft tissue profile.
Before fixed Orthodontics, retained deciduous canines were extracted to allow eruption of permanent canines. Following that rapid palatal expansion of constricted maxilla using fan shaped expander was done (Figure 5). The activation protocol was one quarter turn twice per day [11]. for three weeks The intercanine width was increased significantly.
 Figure 5: Fan shaped expander a) Before expansion b) After expansion
Figure 5: Fan shaped expander a) Before expansion b) After expansion
The fixed orthodontic treatment was planned using preadjusted edgewise appliance and MBT prescription 0.022x0.28 inch slot. Initial upper bonding was done. After 18 months of retention phase of expansion fan shaped expander was removed and lower bonding was done. Wire sequence of 0.014, 0.016, 0.016 x 0:022, 0.017 x 0.025 inch NiTi, 0.019 x 0.025 inch SS were engaged for initial leveling and alignment following which short elastomeric chain was used to close small interdental spaces. After 34 months of active treatment fixed appliance was removed. For retention bonded lingual retainer was given on palatal and lingual surface of anterior six teeth along with hawley’s retainer. Composite build up wrt upper right central incisor was done for aesthetic significance. The post treatment photographs showed significant improvement in the facial profile and both the arches. (Figure 6).

Figure 6: Post-treatment extraoral and intraoral photographs
Case II
A female patient aged 15 years reported to Department of Orthodontics and Dentofacial Orthopaedics with chief complaint of irregularly placed upper and lower front teeth. She has no significant habit history. Extraoral examination showed a symmetrical face, convex profile, obtuse nasolabial angle, average growth pattern and competent lips (Figure 6). Smile analysis found a non-consonant smile arc and visible buccal corridors. Lower dental midline was shifted to left by 2mm. On functional examination she had a forward path of closure. Intraorally, she had a class I molar relation on the left side and right side with overjet of 3 mm and overbite of 3 mm. Crossbite was present wrt upper right and left canine. The upper and lower anterior teeth had a moderate amount of crowding with multiple rotations. She had a narrow V-shaped maxillary arch (Figure 7).
 Figure 7: Pre-treatment extraoral and intraoral photographs
Figure 7: Pre-treatment extraoral and intraoral photographs
Cephalometric analysis showed a Class I skeletal jaw base (ANB angle = 2°), average mandibular plane angle (FMA = 28o). On dental analysis, she had proclined upper and upright lower incisors (U1-NA = 25/5° and L1-NB = 23/3°). The panoramic radiograph showed all teeth present with no mandibular asymmetry with normal shape and size of the condyles with apparently equal ramal and body length bilaterally. No pathological radiopacity/ radiolucency seen (Figure 8).
Figure 8: Pre-treatment lateral cephalogram and panaromic radiograph
Occlusal radiograph showed stage D of mid-palatal suture ossification (Figure 9). Ashley howe analysis showed premolar basal arch width (PMBAW) is more than Premolar diameter (PMD) so it was an indication that basal arch is sufficient to allow expansion.
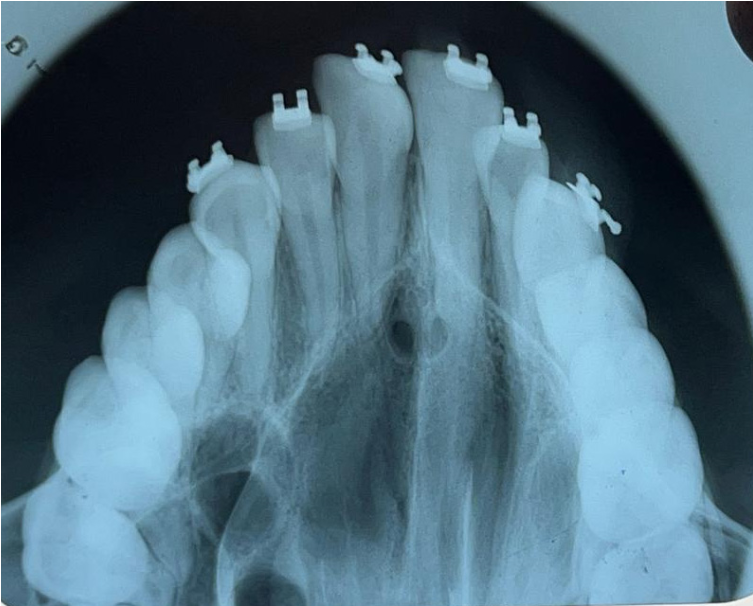
Figure 9: Pre-treatment occlusal radiograph
The main objective of orthodontic treatment was expansion of constricted maxillary arch and to correct crowding in upper and lower anteriors with achievement of Class I canine and Class I molar relationship on both the sides achieving harmonious soft tissue profile.
Before fixed Orthodontics, rapid palatal expansion of constricted maxilla using fan shaped expander was done (Figure 10). The activation protocol was one quarter turn per day [11] for 3 weeks.
 Figure 10: Fan shaped expander a) Before expansion b) After expansion
Figure 10: Fan shaped expander a) Before expansion b) After expansion
Occlusal radiograph of before and after expansion shows significant increase in intercanine width. (Figure 11).
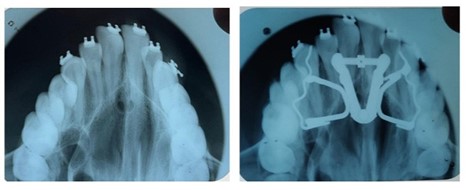 Figure 11: Occlusal radiograph a) Before expansion b) After expansion
Figure 11: Occlusal radiograph a) Before expansion b) After expansion
Discussion
A palatal sutural expansion is necessary if there is a discrepancy in the transverse dimensions of the upper jaw and denture base. One unique characteristic of sutures is that, following orthopaedic therapy, these structures regenerate rather than creating scar tissue or repair tissue [12]. This is comparable to how the periodontal ligament reacts to orthodontic force. Selective anterior expansion is necessary in patients with narrow maxilla, particularly if there is normal molar width and no posterior crossbite. When the standard RME screw is used the cuspid area and molars expand almost parallelly and the arch is extended in the area where it is not necessary. To overcome, Schellino et al [10]. gave the fan-type RME. When Doruk et al [13]. examined the effects of tissueborne fan-type RME with Hyrax, they found that fan-type RME had significantly more intercanine expansion than Hyrax. According to Luca Levrini and Filippi [14] a narrow maxilla case that was treated with fan-type RME showed more intercanine expansion growth than intermolar expansion. In both case reports I and II patient have good occlusion in molar region, and both have narrow constricted ‘V’ shaped arches and decreased intercanine width. That’s why a fan shaped expander was chosen and placed in anterior region and the arms of expander was soldered to framework. After 3 weeks of activation one quarter turn per day expansion was achieved. In case I increase in intercanine width also gained space which was required for buccally erupting canine. In case II increase in intercanine width helped to correct crossbite of left and right canine. Also minimal dentoalveolar tipping and expansion was seen in posterior molar region.
Conclusion
The outcome suggest that in case of anterior narrow maxilla, fan shaped expander helps in expanding maxilla both dental and skeletally anteriorly with minimal posterior changes. Further more studies are required to understand any anterio-posterior changes produced by fan-shaped screw.
References
1. Proffit, W.R. Multicenter, Internet-Based Orthodontic Education: A Research Proposal. Am. J. Orthod. Dentofac. Orthop. 2005, 127, 164–167. [CrossRef] [PubMed]
2. Iodice, G.; Danzi, G.; Cimino, R.; Paduano, S.; Michelotti, A. Association between posterior crossbite, skeletal, and muscle asymmetry: A systematic review. Eur. J. Orthod. 2016, 38, 638–651. [CrossRef] 7.
3. Cossellu, G.; Biagi, R.; Faggioni, G.; Farronato, G. Orthodontic Treatment of Binder Syndrome: A Case Report with 5 Years of Follow-up. Cleft Palate Craniofac. J. 2015, 52, 484–488. [CrossRef] 8.
4. Cossellu, G.; Farronato, G.; Nicotera, O.; Biagi, R. Transverse maxillary deficit and its influence on the cervical vertebrae maturation index. Eur. J. Paediatr. Dent. 2016, 17, 147–150.
5. Persson M, Thilander B. Palatal suture closure in man from 15 to 35 years of age. Am J Orthod. 1977;72:42-52
6. Bjork A, Skieller V. Growth in width of the maxilla by the implant method. Scand J Plast Reconst Surgery. 1974; 8-22-33.
7. Bucci, R.; D’Antò, V.; Rongo, R.; Valletta, R.; Martina, R.; Michelotti, A. Dental and Skeletal Effects of Palatal Expansion Techniques: A Systematic Review of the Current Evidence from Systematic Reviews and Meta Analyses. J. Oral Rehabil. 2016, 43, 543–564. [CrossRef]
8. Angell, D.H. Treatment of Irregularity of the Permanent or Adult Teeth. Dent. Cosm. 1860, 1, 540–544.
9. Hicks EP. Slow maxillary expansion: a clinical study of the skeletal versus dental response to low magnitude force. American journal of Orthodontics. 1978 Feb 1;73(2):121-41.
10. Schellino E, Modica R, Benech A, Modaro E. REM: The spider lives according to Schellino and Modica. Boll Interm Orthod. Leone 1996;55:36-9.
11. Carlson C, Sung J, McComb RW, Machado AW, Moon W. Microimplant-assisted rapid palatal expansion appliance to orthopedically correct transverse maxillary deficiency in an adult. Am J Orthod Dentofacial Orthop. 2016 May;149(5):716-28. doi: 10.1016/j.ajodo.2015.04.043. PMID: 27131254.
12. Ten Cate AR, Freeman E, Dickinson JB. Sutural development: Structure and its response to rapid expansion. Am J Orthod 1977;71:622-36.
13. Doruk C, Bicakci AA, Basciftci FA, Agar U, Babacan H. A comparison of the effects of rapid maxillary expansion and fan-type rapid maxillary expansion on dentofacial structures. Angle Orthod 2004;74:184-94.
14. Levrini L, Filippi V. A fan-shaped maxillary expander. J Clin Orthod 1999;33:642-3.
This article licensed under the Creative Commons Attribution 4.0 International License CC-BY 4.0., which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are properly credited.