
NL Journal of Dentistry and Oral Sciences
(ISSN: 3049-1053)
The Keys to Succeed Immediate Dentures: A Case Report
Author(s) : Chtioui Hajer, Bekri Sana, Zidani Hajer, Ouni Imed, Mansour Lamia. DOI : 10.71168/NDO.01.01.110
Abstract
An immediate denture is a complete denture or removable partial denture fabricated for placement immediately after tooth extraction due to esthetic reasons. It is used to enhance esthetics, protect extraction related surgical wound and provide function during healing. It also preserves oral support, bone, muscle tone, vertical dimension of occlusion, jaw relationship, and face height. In this article, we describe the use of indices served to record the current position of the remaining dentition, it can then be decided if this is to be reproduced in the denture or if teeth have drifted, extruded and they are to be restored to the original position. Keywords: Immediate denture, aesthetic denture, transitional, anterior teeth extraction.
Introduction
An immediate complete denture is a restoration fabricated prior to the extraction of a tooth, which is placed in the patient’s mouth immediately following the removal of the remaining teeth [1].
The main advantages of immediate dentures are maintained aesthetics, digestive function stays uninterrupted, masticator and facial muscles do not change, bone support is maintained, it controls hemorrhage, prevents contamination, and psychological benefits [1-2].
The success of immediate dentures depends on the correct indication and precise execution of clinical and laboratory fabrication procedures. The description, step by step, of the imperatives to follow to succeed in the prosthetic project has been developed through a clinical case.
Case Report
Mr. H, 45 years old, in good general health, came to consult the partial removable denture department in the Dental clinic in Monastir Tunisia for aesthetic and functional prosthetic restoration.
The extraoral clinical examination did not reveal any notorious peculiarity neither on inspection nor on palpation The history of the oral situation revealed the extraction of several teeth due to caries and periodontal disease.
The endobuccal examination illustrated poor oral hygiene, and teeth mobility that disturbs the patient during function and Recessions. (Fig1)
 Figure 1: Initial clinical situation and panoramic x-ray
Figure 1: Initial clinical situation and panoramic x-ray
The panoramic radiological examination revealed a generalized alveolysis, sign of severe periodontal disease, and the residual maxillary teeth have a radiological crown / radiological root ratio >1 (Fig1)
Debridement of the existing teeth should be done with an initial prophylaxis followed by oral hygiene instructions. A hygiene motivation was made.
The therapeutic decision was an immediate maxillary denture to ensure the aesthetic demand of the patient and to maintain oral functions.
We started with the extraction of the posterior maxillary teeth mobile degree 2, the patient’s posterior teeth should be removed as soon as possible. These posterior extraction and other operated areas are allowed to heal for a short time usually 3 to 4 weeks.
Preliminary impressions were made for two primary reasons. The first is to use these impressions in the fabrication of casts that will be used in diagnosis and treatment planning. The second purpose is for the fabrication of custom impression trays. The diagnostic impressions were made using an irreversible hydrocolloid material and models were obtained using Dental Plaster.
After the assembly of the diagnostic casts, an egression of the mandibular incisor was noted, and a 1mm grinding of the mandibular incisor edge was carried out. (Fig 2)

Figure 2: Grinding of the lower incisors to restore the occlusal plane
It was supported by an individual impression tray made from a primary model. Given the mobility of the teeth and the presence of retentive areas, the impression tray made of cold-curing acrylic resin was windowed facing the teeth and combined with a removable cover. (Fig 3)
 Figure 3: Perforated individual impression tray
Figure 3: Perforated individual impression tray
The individual impression tray had been set and adjusted in the mouth, eliminating any interference. The seals posteriorly as well as in the lateral edentulous areas were recorded with Kerr® thermoplastic paste in the same way as in a conventional full denture. In the anterior dentulous region, a “soft seal” was made with a polyether that allows precise registration of the functional anterior limit, without overextension or over-thickness, the impression was carried out using polysulfer regular.
The plaster silicone key materializes the situation of the anterior occlusion plan and memories the anterior space situation teeth. (Fig 4)
 Figure 4: Secondary working impression
Figure 4: Secondary working impression
Maxillomandibular relationship records careful assessment of the dentition in the opposing arch must be made and any alterations in its form, so as to establish a more favorable occlusion. The centric relation record is made directly at the established vertical dimension.
The articulated casts were used for setting posterior teeth that were missing. Set the teeth in centric occlusion Posterior Teeth Setup for Wax Try-in. (fig 5)

Figure 5: Posterior Tooth Setup for Wax Try-in
The posterior teeth already had been arranged; consequently, the remaining teeth may be removed from the stone cast and the cast adjusted to simulate the soft and hard tissue contours that would be anticipated following removal of teeth. Verification of the position of the occlusion plan by the silicone key (Fig6)
 Figure 6: Extraction sites trimmed, Teeth setup, and wax up
Figure 6: Extraction sites trimmed, Teeth setup, and wax up
A surgical guide was performed, it was used to guide for surgical shaping of the alveolar process. (Fig 7)
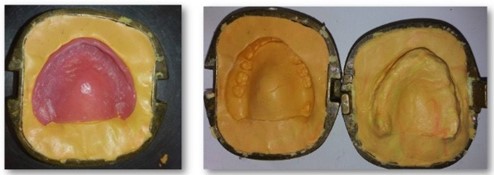 Figure 7: Fabrication of the Surgical guide based on the wax denture setup
Figure 7: Fabrication of the Surgical guide based on the wax denture setup
Tooth removal was performed carefully to maintain the integrity of the bony plates, surgical template will be inserted before closure of the surgical site and any areas of tissue blanching, which will be evident through the clear template, should be corrected by minor alveoloplasty. A labial frenectomy was made. (Fig 8 and 9)
 Figure 8: Dental extraction, regularization of alveolar Crete, frenectomy
Figure 8: Dental extraction, regularization of alveolar Crete, frenectomy
 Figure 9: Surgical guide
Figure 9: Surgical guide
The prosthesis had been put in the mouth and occlusal equilibration was carried out, the denture was garnished by a conditioner (fit de kerr) which will guide healing and amortize shocks (Fig 10 and 11)
 Figure 10: Delivery of the prosthesis
Figure 10: Delivery of the prosthesis

Figure 11: Delayed-setting resin for the prosthetic intrados
The patient will be seen in 24 hours to evaluate denture retention, support, and stability. After 1 week, sutures can be removed, and the patient can begin removing the denture at night.
After complete healing, the prosthesis can be relined or redone.
Discussion
Immediate dentures are fabricated increasingly nowadays, mainly for aesthetic and psychological reasons.
It can be a transitional denture immediately used for a short interval of time for aesthetics and functional reasons until more definitive prosthetic therapy can be provided, it can be a conventional immediate denture which can be later rebased to serve as the permanent prosthesis, also it can be diagnostic dentures [3-4].
Gooya et al. (2013) used the patient’s fixed prosthesis for fabricating an interim immediate partial denture in one appointment, by maintaining the VDO. He concluded that the present occlusion, VDO and facial support could be maintained during the healing period in this procedure [5].
Throughout the impressions, the presence of dental mobility made it necessary to fill these spaces with pink wax or high viscosity silicone to avoid tearing of the material and possible periodontal lesions to the mobile teeth [6].
The anatomy functional impression was taken using light silicone and a windowed individual tray. In fact, the light silicone is a fluid material during insertion but elastic after setting what allows easy removal of the impression without traumatizing teeth [7].
As for the windowed impression tray, it has the advantage of ensuring comfort for the patient during the physiological registration of the peripheral joint as well as a smooth demolding of the Master Cast without fracturing the teeth in the laboratory [8].
the application of a tissue conditioner in the intrados of the prosthesis after surgery improves comfort of the patient during the healing by providing a better peripheral seal, as a result a better retention, and softening the occlusal forces transmitted by the prosthesis to the underlying tissues [9].
At last, maintenance is essential to ensure the integration of the prosthesis in the medium and long term [10].
Conclusion
The realization of an immediate complete removable prosthesis requires establishing a good protocol, from the start to the follow -up sessions. Some steps remain common to the realization of the complete conventional prosthesis, however, the anticipation of difficulties specific to the immediate prosthesis and their management are indispensable to ensure maximum success.
References
1. Krati Sharma, Punit Raj Singh Khurana, Vishwas Bhatia, Priyanka. Fabrication of an Immediate Denture: A Case Report International Journal of Science and Healthcare Research Vol.5; Issue: 1; Jan.-March 2020
2. DiptiNayak, RomilSinghal and col IMMEDIATE DENTURE: A REVIEW , INTERNATIONAL JOURNAL OF SCIENTIFIC RESEARCH Volume-9 | Issue-2 | February-2020 | PRINT ISSN No. 2277 – 8179
3. Gilboa I, Cardash HS. An alternative approach to the immediate overdenture. J Prosthodont 2009; 18:71-5.
4. Heartwell, cm, jr., and salisburyfw. Immediate complete dentures: an evaluation. J Prosthet Dent 1965;15(4):615-24.
5. Gooya A, Ejlali M, Adli AR. Fabricating an interim immediate partial denture in one appointment (modified jiffy denture). A clinical report. J Prosthodont.2013; 22:330- 3
6. Regragui A, Abdedine A, Sefrioui, Merzouk N. Les causes d’echec en prothèse amovible complète d’usage. Web J Dent. 2(4).
7. Rignon-Bret C, La prothèse complete immédiate:données actuelles Stratégie prothétique. Stratégie prothétique. 2016;16(4).
8. Abdelkoui A, Fajri L, Benamar A, Abdedine A. La prothèse complète immédiate d’usage: Réalisation temps par temps. Clinic. 2013;34: 87-95.
9. Postaire M, Pompignoli M. Les dernières dents... Garder ou extraire: solutions cliniques. Paris: Information Dentaire; 2011.
10. Guessous DF., Fajri L., Merzouk N. Réhabilitation esthétique et fonctionnelle par PACIU dans un cas de classe II squelletique.AOS n° 280 – 2016
This article licensed under the Creative Commons Attribution 4.0 International License CC-BY 4.0., which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are properly credited.