
NL Journal of Dentistry and Oral Sciences
(ISSN: 3049-1053)
Pediatric Enigma: A Case Report of Ossifying Fibroma
Author(s) : Dipanwita Chakraborty, Sunitha Bhosle, Mahalakshmi Wale. DOI : 10.71168/NDO.01.01.109
Abstract
Juvenile ossifying fibroma is a rare, aggressive, benign fibro-osseous lesion, typically discovered early as a bony overgrowth, often without symptoms. The recurrence rate for this condition is quite high. This article presents a case of juvenile ossifying fibroma in a 6-year-old male patient. Upon clinical examination, a solitary growth on the right side of the patient’s face was observed. A panoramic radiograph, postero-anterior skull view radiograph, and CT scan were performed. Complete excision with hemi-maxillectomy of the growth was carried out, followed by surgical reconstruction using an autogenous graft. Biopsy revealed a fibro-osseous lesion, and the diagnosis given was Juvenile trabecular ossifying fibroma. Keywords: Juvenile trabecular ossifying Fibroma, Fibro-osseous lesion, Recurrence.
Introduction
Benign fibro-osseous lesions are uncommon in the head and neck region and can include various tumors with similar characteristics. These tumors encompass fibrous dysplasia (FD), ossifying fibroma (OF), and cementoosseous dysplasia (COD) [1]. Ossifying fibroma can be categorized into conventional and juvenile forms (JOF). According to the World Health Organization (WHO) classification of odontogenic tumors 2005, JOF is further divided into juvenile psammomatoid ossifying fibroma (JPOF) and juvenile trabecular ossifying fibroma (JTOF). The psammamatous type usually affects the bones of the orbit and paranasal sinuses, while the trabecular type commonly impacts the jaws [2]. The preferred treatment is complete surgical removal. JOF has a notable recurrence rate after treatment. The specific age of occurrence in younger individuals, location, histological variability, and potential for aggressive behavior contribute to the unique nature of juvenile ossifying fibroma.
Case Presentation
A 6-year-old male patient visited the Oral Medicine and Radiology department of a dental college in Karnataka with a chief complaint of swelling on the right side of the face persisting for three months. The patient’s parents reported a history of a fall four months prior, for which they did not seek medical assistance. Around one month after the fall, they noticed a small swelling on the right side of the patient’s face, which gradually increased to the current size. There was no history of pain or paresthesia in that region. The patient’s medical, dental, and family histories were unremarkable. The patient was poorly built and moderately nourished. All of the vital signs of the patient were normal. Figure 1: 6-year-old male patient with a notable growth on the right side of the face
Figure 1: 6-year-old male patient with a notable growth on the right side of the face
 Figure 2: Intra-oral diffuse swelling at the right palatal region
Figure 2: Intra-oral diffuse swelling at the right palatal region
During the clinical examination, a well-circumscribed growth was observed on the right side of the face, [Figure 1] extending from the nasal bridge to one cm away from the posterior border of the mandible and from 0.5 cm short of the infraorbital rim to one cm short of the inferior border of the mandible. The growth measured 6x5 cm² in diameter. Upon palpation, there was a local rise in temperature over the growth, it was firm to hard in consistency and non-tender. Intra-orally, a diffuse swelling was found on the right palatal aspect extending from one cm away from the palatal rugae to the junction of the soft and hard palate and 0.5 cm away from the mid palatine raphe to the mucogingival junction on the right palatal side. [Figure 2]. The overlying mucosa of the intra-oral swelling was normal, non-tender on palpation, and firm to hard in consistency. Grade I mobility was felt on percussion concerning teeth 53, 54, and 55. The provisional diagnosis was central giant cell granuloma involving the right side of the face. The differential diagnoses included mono-ostotic fibrous dysplasia, ameloblastoma, central hemangioma, ossifying fibroma, giant cell tumor of bone, and odontogenic myxoma.
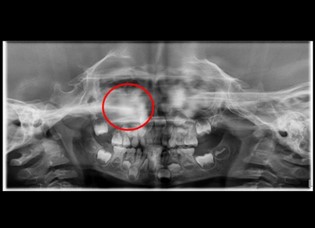 Figure 3: OPG of the patient
Figure 3: OPG of the patient
 Figure 4: PA Skull view revealing an ill-defined shadow in the maxillary sinus
Figure 4: PA Skull view revealing an ill-defined shadow in the maxillary sinus
The patient was advised to undergo an OPG [Figure 3] and a postero-anterior view radiography [Figure 4] of the skull. Both images revealed an indistinct opaque area in the right maxillary sinus region, extending into the nasal cavity and causing displacement of the lateral wall of the nose and into the infra-orbital rim. The internal structure of the maxillary sinus appeared as a poorly mixed opaque and radiolucent area.
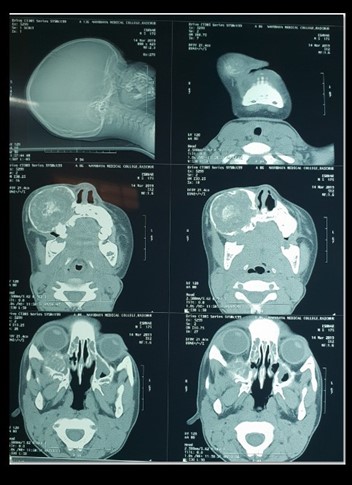 Figure 5: CT scan of head and neck revealed a large expansile circumscribed lesion involving the maxillary alveolus on the right side and maxillary sinus
Figure 5: CT scan of head and neck revealed a large expansile circumscribed lesion involving the maxillary alveolus on the right side and maxillary sinus
To better understand the extent of the growth, a CT scan [Figure 5] was recommended, revealing a large expansile circumscribed area involving the maxillary alveolus on the right side and the maxillary sinus, with a thick opaque border. The growth extended into the nasal cavity, causing deviation of the right inferior and superior turbinate. The centre of the growth appeared as a mixture of radio-opaque and radiolucent structures. Displacement of the inferior wall of the orbital rim was also observed.
 Figure 6: Excised specimen
Figure 6: Excised specimen
The growth was completely excised with right hemimaxillectomy under general anaesthesia. [Figure 6]. Surgical reconstruction was performed using an autogenous graft. On gross examination, the specimen appeared as a bony hard mass. Microscopically, the H&E stained sections showed spindle to oval shaped cells forming fascicles in some areas and interspersed with numerous areas of mineralized components.
Based on the clinical presentation, radiological and histopathological findings, the growth was diagnosed as Juvenile trabecular ossifying Fibroma. An interdisciplinary team comprising of oral physicians, oral surgeons, prosthodontists, and paedodontists was formed. Following the surgery, the patient was restricted from taking anything by mouth for the next 24 hours. The prescribed medications included intravenous (I.V) fluids Isolyte-p at 20ml/hour for 2 days, injection Ceftriaxone 500mg (I.V) twice a day for 5 days, injection metronidazole 20ml I.V twice a day for 3 days, injection dexamethasone 4mg once a day for 7 days, and injection paracetamol 20ml thrice a day for 5 days.
A palatal obturator was placed after consultation with the prosthodontists of the team to improve the general appearance, articulation, speech, mastication, and deglutition of the patient.
The patient was followed up for the next year after the surgery. No adverse events related to the medications and no recurrence were reported during the 1 year follow-up period.
Discussion
Juvenile Ossifying Fibroma (JOF) is a rare and aggressive fibro-osseous entity. JOF has an osteolytic nature due to intense osteoblastic activity and can resemble a malignant tumor [3].
The histopathological definition of Juvenile Trabecular Ossifying Fibroma describes it as an unencapsulated tumor with a hypercellular stroma composed of spindle cells, with minimal collagen production, and with long slender strands of osteoid. [10] On the other hand, Juvenile Psammatomatous Ossifying Fibroma is an unencapsulated tumor containing multiple irregular and spherical psammomatoid basophilic bodies with a concentric pattern of lamination embedded in cellular fibroblastic stroma.
JOF is typically observed in individuals under 15 years of age, with a slightly higher incidence in males. The tumor is usually large and expansile, frequently extending into the ethmoid and sphenoid sinuses, the nasal cavity, orbital walls, and maxillary bone [9]. Mandibular lesions are also observed.
Clinically, JOF may manifest as an asymptomatic gradual or rapid expansion of the affected bone, leading to facial asymmetry. Proptosis is another common clinical symptom. Other symptoms may include headaches, pain, recurrent sinusitis, and nasal obstruction lasting from several weeks to several months. Missing teeth may also occur due to disruption in the formation of tooth sockets.
Radiographically, juvenile ossifying fibroma (JOF) displays well-defined borders with thin radiolucency that separates it from the surrounding bone. The internal structure of JOF can be radiolucent, mixed, or radiopaque depending on the degree of calcification. JOF may displace a tooth or the inferior alveolar canal, depending on its location. For a better understanding of these lesions, CT and MRI scans may be recommended to the patient, which can also assist in treatment. CT scans play a crucial role in the differential diagnosis of conventional adult ossifying fibroma, fibrous dysplasia, and cemento-osseous dysplasia. While juvenile ossifying fibroma typically exhibits CT changes akin to the conventional form, it can occasionally present in a more aggressive manner, featuring cortical destruction. Magnetic resonance imaging is essential for evaluating the extent of the lesion, although it is less effective in clearly delineating its bony components [4,8].
The treatment of JOF can be either conservative or aggressive, depending on the behaviour of the lesion. Nonaggressive forms of JOF can be managed by curettage and local surgical excision. Aggressive lesions, characterized by rapid growth, thinning, or perforation of cortical bone, tooth displacement, or root resorption, may exhibit early recurrence [6]. Therefore, block resection is warranted when extremely aggressive behaviour is observed [5].
The high recurrence rate of JOF is primarily linked to incomplete excision stemming from the infiltrative nature of the tumor’s borders. Consequently, enucleation followed by peripheral osteotomy is the definitive treatment of choice for both variants of JOF. This approach effectively minimizes the disfigurement commonly associated with surgical resection. It is essential to excise the tumor mass down to the level of normal bone while preserving adjacent vital structures whenever possible [7].
In the present case scenario, scar formation on the right side of the face due to the extra-oral surgical approach could be an esthetical concern for the patient. As hemi-maxillectomy was done, and the patient was on a liquid diet for the next 2 months after surgery, which in turn affected his general health.
The parents of the patient were pleased with the surgical outcome. However, they were understandably concerned about the possibility of the lesion recurring. They expressed their heartfelt wish for their son to remain free from the condition for the rest of his life.
Conclusion
Juvenile ossifying fibroma is aggressive and highly recurring (30-58%), so early diagnosis is essential for treatment planning. Long-term follow-up is recommended to monitor recurrences, and psychological counselling is advised to support patients’ mental well-being.
References
1. Sarode SC, Sarode GS, Waknis P, Patil A, Jashika M. Juvenile psammomatoid ossifying fibroma: a review. Oral oncology. 2011 Dec 1;47(12):1110-6.
2. Smith SF, Newman L, Walker DM, Papadopoulos H. Juvenile aggressive psammomatoid ossifying fibroma: an interesting, challenging, and unusual case report and review of the literature. Journal of oral and maxillofacial surgery. 2009 Jan 1;67(1):200-6.
3. Breheret R, Jeufroya C, Cassagnaub E, Malardc O. Juvenileossifying fibroma of the maxilla. European Annals of Otorhinolaryngology, Head and Neck diseases. 2011.
4. Khoury NJ, Naffaa LN, Shabb NS, Haddad MC. Juvenile ossifying fibroma: CT and MR findings. European radiology. 2002 Dec;12(3):S109-13.
5. Abuzinada S, Alyamani A. Management of juvenile ossifying fibroma in the maxilla and mandible. Journal of maxillofacial and oral surgery. 2010 Mar 1;9(1):91-5.
6. Noffke CE. Juvenile ossifying fibroma of the mandible. An 8 year radiological follow-up. Dentomaxillofacial Radiology. 1998 Nov 1;27(6):363-6.
7. Chrcanovic BR, Gomez RS. Juvenile ossifying fibroma of the jaws and paranasal sinuses: a systematic review of the cases reported in the literature. International journal of oral and maxillofacial surgery. 2020 Jan 1;49(1):28-37.
8. Kawaguchi M, Kato H, Miyazaki T, Kato K, Hatakeyama D, Mizuta K, Aoki M, Matsuo M. CT and MR imaging characteristics of histological subtypes of head and neck ossifying fibroma. Dentomaxillofacial Radiology. 2018 Sep;47(6):20180085.
9. Ollfa BG, Nadia R, Safa N, Madiha M, Wafa A, Ines H, Chiraz MC. Juvenile ossifying fibroma of the maxilla. Egyptian Journal of Ear, Nose, Throat and Allied Sciences. 2017 Jul 1;18(2):145-9.
10. Osunde OD, Iyogun CA, Adebola RA. Juvenile aggressive ossifying fibroma of the maxilla: a case report and review of the literature. Annals of medical and health sciences research. 2013 Apr;3(2):288.
This article licensed under the Creative Commons Attribution 4.0 International License CC-BY 4.0., which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are properly credited.