
NL Journal of Dentistry and Oral Sciences
(ISSN: 3049-1053)
Evaluation of Costal Cartilage and Restore the Function in Treatment of Temporomandibular Joint Immobility
Author(s) : Reda Ahmed Nofal. DOI : 10.71168/NDO.01.01.104
Abstract
The aim of this work was to assess the Inter positional graft after the release of a bony union of the temporomandibular join. 14 patients with bony union of the temporomandibular joint were selected. In these patients, they replaced with Interposition material, and the patients were followed clinically and radiographically for 10 months. Of the 15 grafts, results of the present study found good remodeling in 10 patients (70%), re ankylosis in 3 patients (20%), and resorption of the graft in 2 patients (10%). The examination of the opening was satisfactory (more than 35mm) in 10 of the 15 patients (67%), unsatisfactory (between 5 and 25mm) in 3 (20%), and the operation was a failure in 2 (13%). This work demonstrated that the Interposition costal cartilage is a suitable material for interposition arthroplasty. The physical rehabilitation appears key element in the success of this procedure. keywords: Bony fusion, Condylar bon glenoid fossa
Introduction
The bony union of the temporomandibular joint (TMJ) involves fusion of the head mandibular condyle to the glenoid fossa and base of the skull, which causes distressing conditions including impaired speech, difficulty in chewing, facial disfigurement, compromise of the airway and psychological stress. This is particularly true in young children who are completely unable to open their mouths. It is usually caused by trauma and infection. The patients with ankylosis of the TMJ and micrognathia, the treatment is often in two parts: trismus can be managed by gap arthroplasty or by reconstruction of the TMJ while the micrognathia can be treated by autoplastic bony transplantation or distraction osteogenesis (DO) [1,18]
Costochondral grafts, which have the advantages of being autogenous material with a cartilaginous articulating surface and the potential for growth and adaption, are commonly used to reconstruct the mandibular condyle. Their disadvantages are the need for an additional operation, which may cause morbidity at the donor site, and an unpredictable pattern of growth [16,17]
The time of the diagnosis, the type of operation, and the policy of treatment vary from one country to another, however, the main principles are the same: (a) satisfactory resection of the ankylotic segment; (b) use of interpositional spacer, if it is needed; (c) early aggressive and insistive postoperative physiotherapy [6,7,8]
Facial asymmetry is the classic feature in unilateral cases, the chin deviates toward the affected side, vertical height of the affected side is shorter when compared with the unaffected side, a complete absence of mouth opening and recession of the chin are typical characteristics of the bilateral ankylosis, the degree of recession and the asymmetry of the mandible depends on the growth situation and the onset of ankylosis [9]
Reconstruction of the mandibular condyle after the release of ankylosis of the temporomandibular joint is a challenging problem in maxillo-facial surgery. A successful reconstruction implies correct restoration of form and, in children, future symmetrical growth [10].
The width of bone removal is crucial, and it is recommended that a minimum gap of 1cm is necessary to prevent re ankylosis. However, this magnitude of the gap will result in an anterior open bite in bilateral cases or a posterior open bite on the contralateral side in unilateral cases [11].
Verneuil (5) was the first to suggest the interposition of muscle and fascia between the bony cuts, and then many of the materials proposed for TMJ arthroplasty: autogenous bone, cartilage muscle, fat dermis, fascia, skin, metatarsal, and sternoclavicular joint. [6; 7; 8] Numerous alloplastic materials have been used for partial or total reconstruction of the TMJ for release of temporomandibular\joint (TMJ) has the advantage of effectively freeing the mandible and avoiding the dense overgrowth of bone high in the condylar [12,13].
When costochondral grafts have been used in children, the subsequent growth of the graft has been unpredictable, and usually excessive. Clinical and radiographic studies have shown no growth in some patients and excessive growth in others and the results are unpredictable. However, encouraging functional and cosmetic results have been reported. Restoration of normal function and jaw movement in patients with TMJ ankylosis is difficult. Various techniques have been defined for the treatment of the condition. Many techniques for treatment have been described so far. However, none of them gave uniformly successful results [14].
A limited range of mouth opening due to relapse, loss of vertical height of the affected ramus, and re ankylosis are expected complications. However, wide bone resection, costochondral grafts, and aggressive physiotherapy immediately after the operation are the basic principles as agreed by many authors [15].
In an attempt to overcome such drawbacks of reconstructing the temporomandibular joint after the release of ankylosis, the costochondral grafts. (1) Although the ideal technique for reconstructing the temporomandibular joint after the release of an ankylosis, is still an issue of controversy, the present study, has hypothesized that gap arthroplasty with costochondral grafts could be of value as a suitable technique for the treatment of temporomandibular joint ankylosis
Aim of the work: This study was conducted clinically, to assess the costochondral grafts that were used to reconstruct the temporomandibular joint after removal the masses of the bony union.
Patients and Methods
There were 15 patients with unilateral ankylosis, who underwent a gap arthroplasty, making a total of 15 costochondral grafts. In 10 the ankylosis was primary and in 5 recurrent was included in the study. The highest incidence was observed in the 12–22 age group 75% followed by the 1–10 age group 25%. The common etiologic factor is Falling accidents during early childhood was 10 in this study and 5 patients had been injured in traffic accidents, Clinical and radiographic examinations by orthopantomogram, lateral cephalograms, and computed tomograms were made pre-operatively after, 4 months, and 1 yearly.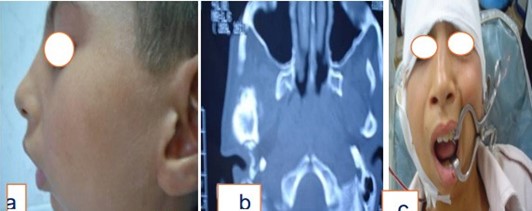
Fig.1. a) Lateral view showing a girl 12 years old with TMG ankylosis.
b) Axial view CT image showing bony fusion in ankylosis and calloused masse
c) Post operative showing the complete opening of the mouth and exercise using mouth gauge
Surgical technique
In this study, all the patients were operated under general anesthesia using fiberoptic endoscopy technique. To approach the TMJ area, a preauricular incision was made, the incision was deepened avoiding injury to the superficial temporal vessels and the facial nerve. The dissection proceeded in this plane to the zygomatic arch and extended anteriorly and posteriorly to expose the limits of the ankylosis. The periosteum over the zygomatic arch and the ramus were incised and elevated. After exposure to the site of bony block, bone was removed by using a round burr until a thin cortical bone was left in the depth. In order not to injure the internal maxillary artery or pterygoid plexus of veins, two segments were gently split and fractured by using a chisel. The irregular edges of the segments were shaved by bur and disconnected completely the ramus from the upper bony block
Preparation of the recipient bed: After the release of ankylosis by condylectomy and coronoidectomy, the glenoid fossa is smoothed using different sizes of carbide rose-head burs with adequate irrigation. If the cartilaginous disc is available, it is retained and repositioned to line the glenoid fossa as in fig 2 and 3.
Harvesting the costochondral graft: The graft is taken from the 5th or 6th ribs. Usually, 3 to 5 cm of bone is harvested with a cap of 5mm of cartilage (fig 2 -3). If two grafts are needed, in bilateral cases, alternate ribs are taken from the same side to avoid a flail chest.
 Fig.2. a) Operative view showing the sub nibble incision for the graft
Fig.2. a) Operative view showing the sub nibble incision for the graft
b) Harvesting the costochondral graft 6th ribs
c) Cartilage costochondral graf still attached to rib
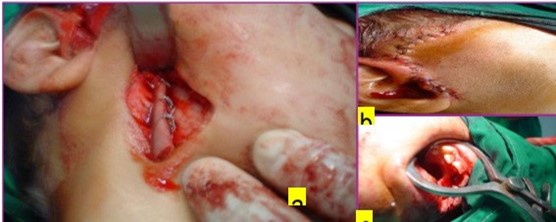
Fig.3. a) Operative view showing fixation of the costochondral graft in place
b)Showing surgical site and interrupted sutures post-operative
c)Normal mouth opening returned normal after gap arthroplasty
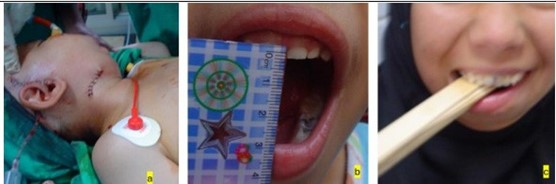
Fig.4. a) Postoperative view showing the submandibular and preauricular approaches.
b) 6 months postoperatively mouth opening was 34
c)Mouth opening exercise, using a bundle of tongue depressors with gradually increasing number
The right side of the chest is preferred for graft, care must be taken to preserve the perichondrium and periosteum at the bone cartilage junction to maintain adequate strength in this potentially fragile area. The graft is trimmed to the required length with a cartilaginous cap 3 to 5mm deep (fig 2-3).
Preparation of the costochondral graft and bed; in children, multiple partial thickness bur holes are made in the surface that lies in contact with the ramus. In adults that surface is decorticated. The recipient surface of the ramus is also decorticated to ensure perfect contact between the two bony surfaces which helps revascularisation and take of the graft (fig 2 -3).
Insertion, orientation, and fixation of the graft; Through a submandibular and extended preauricular incision, the graft is inserted and oriented on the lateral surface of the ramus as the only graft with about 5mm of space left in the glenoid fossa to permit free condylar movement (fig 2 -3).
The graft is fixed to the ramus by wires or bone screws. If the graft is fixed with screws the mandible is released immediately after unilateral operation and after a week after bilateral operation. Two or three 9-11mm mini- screws are adequate for fixation in adults and 7-9mm mini-screws in children. However, there is a hazard that they may cause a longitudinal fracture of the fragile graft particularly in children and the marrow may extrude through the lower end of the graft as the screws are tightened. Extreme care must be taken to avoid malpositioning or displacement of the posterior border of the ramus is not advised because in long-standing ankylosis the ramus is usually deformed, and adequate bony contact between the graft and the ramus is difficult to achieve (fig 2 -3).
Fixation of the graft to the posterior border of the ramus may also lead to more narrowing of the retro- ramal area which is already narrow as a result of long-standing ankylosis and retrognathia. In two patients with recurrent ankylosis, we found the graft fused to the styloid processes.
Post-operative care of the grafts: It is essential to retain maxillo-mandibuar fixation to prevent early and excessive stress loading during the take of the graft, after release of maxillo-mandibular fixation; gradual gentle mouth opening exercises are started, (Fig 4)
All the patients were encouraged to exercise intensively by opening and closing their mandible. The physiotherapy was painful in the first week, but most of the patients showed gradual progress during this time. The gags were used to help and increase mouth opening, for this purpose, different size of wooden gags was used, both passive and active exercises were prescribed according to the patient’s tolerance, a soft diet is recommended for at least a month, forcible opening of the mouth is avoided for at least 6 months to allow for complete bone remodeling. Intermaxillary fixation (IMF) for 2 weeks is recommended, and then assisted mouth opening begins and continues for a minimum of 6 months.
Results
15 patients were included in this study. There were 10 males and 5 females. Following the surgical release of ankylosis the assisted mouth opening achieved ranged from 27 to 49 mm (mean 36 mm)). The highest incidence was between the ages of 12 and 22. Retruded chin was the most common clinical finding, followed by facial asymmetry and midline shift. All the patients except for a few of them were from rural areas and their economic and cultural levels were poor.
Relevantly, the expectation of the patient and his/her family was only the opening of the jaw and the ability of mastication. The complication of immediate postoperative VII nerve weakness was encountered in 20% of cases, there were no instances of pneumothorax or pleural perforation
In 10 patients (66.66%) mouth opening was judged to be satisfactory (more than 26mm) at a minimum of 1-year follow-up, 3 patients (20%) had unsatisfactory mouth opening (between 5 and 25mm) and the remaining 2 patients (12%) had evidence of recurrent ankylosis, these were in accordance with (Hoffman 2023)
All patients in the latter group had presented initially with recurrent ankylosis, and in some patients, there was a history of multiple recurrences. Radiographic studies showed that; 10 grafts (66.7%) had integrated and remodeled satisfactorily, 3 grafts (20%) had resorbed, 2 had bony ankylosis (12%)
Only 2 of the 15 patients who had gap arthroplasty needed a second operation; these were the patients who rejected the early aggressive physiotherapy and regular postoperative controls. Interincisal mouth opening improved considerably postoperatively Follow-up period postoperatively donor site morbidity was low apart from local pain.
Discussion
The current work may lend support to the previous thought that, the early postoperative status of costochondral grafts is difficult to establish because the cartilaginous portion is radiolucent and particularly in children, the rib is poorly calcified, and the graft may not be easily identifiable. This is agreed with [5].
The results of the present study showed that the costochondral grafts have several advantages in that they are autogenous material with a cartilaginous articulating surface that mimics the normal Follow up of mandibular [4].
Clinical observation of the current study showed that to maximize the chance of survival of the graft, the rib should be harvested immediately before being inserted, the recipient bed should be adequately vascularised (there should have been neither previous operation nor irradiation), and the graft should be of the correct length and, early and excessive loading should be avoided. This finding was corroborated by [3].
Not surprisingly, the results showed greater improvement with time the rib becomes assimilated into the ramus. Expectedly, the fragile junction between cartilage and bone may fracture as a result of trauma or vigorous exercises. This can result in dysfunction of the joint that requires surgical intervention This finding was in accordance with that of [1,2]
This study demonstrated that the pattern of growth of the rib graft is unpredictable. In most children, the growth exceeds that of the normal condyle until the two become equal, after which the two sides develop in harmony. In some adults and children, however, the graft does not grow, and the benefits of operation are restricted to the restitution of normal function of the joint. In other cases, the graft can overgrow [14,15].
The current study showed that the costochondral junction, like the mandibular condyle, is a secondary growth site that responds to Passive mouth opening exercise, using a bundle of tongue depressors with a gradual increasing number, to enlargement of the surrounding functional matrix. Growth of the rib can also be affected by various intrinsic hormonal factors which can result in hyperplasia of the graft in a child [19].
Regarding the size of the grafted cartilaginous cap and its relation to growth, little attention has been paid to the size of the grafted cartilaginous cap and its relation to growth. Some hold that a large cap (2.7 cm) is necessary to promote future growth and to prevent re ankylosis. (8) Others argue that a smaller cap; 2-5mm prevents a fracture at the costochondral junction and may play a part in diminishing the potential for overgrowth of the graft. The current study used a cartilaginous cap of 4-6mm in all. Experimental findings support the clinical experience that the outcome is better with a small cartilaginous cap [20].
Conclusion
Based on the findings of the current study, the following conclusions could be drawn; Functional results obtained through the use of gap arthroplasty with costal graft supplemented with active jaw opening exercises, are satisfactory. A gap of 4–5 mm is adequate and early exercise is possible. Consideration is given to the width and level of gap arthroplasty, and fixation of the grafts. This study demonstrated that autogenous costal cartilage is a suitable material for interposition arthroplasty. Close follow-up of the patient and physical therapy play important roles in the prevention of postoperative adhesions and re-ankylosis and further studies on the long-term fate of the cartilage insert are needed following periods of functional loading.
References
1. Mahajan A, Soni D, Dholabhai P, Daithankar S, Shah A, Adalja C. Is Gap Arthroplasty Sufficient in TMJ Ankylosis: Our Experience. The Traumaxilla. 2023;5(1-3):15 19.doi:10.1177/26323273231221250
2. E. Bach, N. Sigaux, M. Fauvernier, A.S. Cousin Reasons for failure of total temporomandibular joint replacement: a systematic review and meta-analysis Int. J. Oral Maxillofac. Surg., 51 (2022), pp. 1059-1068, 10.1016/j. ijom.2021.12.012
3. Bazsefidpay N, Ulmner M, Lund B. Did temporomandibular gap arthroplasty with temporalis interpositional flap improve function and pain in patients with end-stage joint disease? A 5-year retrospective follow-up. J Craniomaxillofac Surg. 2024 May;52(5):578-584. doi: 10.1016/j.jcms.2024.02.013. Epub 2024 Feb 5. PMID: 38368213.
4. Medra A M.M. Follow up of mandibular costochondral grafts after release of ankylosis; British Journal of Oral and Maxillofacial Surgery (2005) 43, 118—122
5. Hoffman DC, Laskin DM. Hyperplasia of a costochondral graft in an adult. J Oral Maxillofac Surg 2004; 5:1392—4.
6. Mactosh RB, Henny FA. Spectrum of application of autogenous costochondral grafts. J Maxillofac Surg 1977;5:257—67.
7. ASowe NL. Ankylosis of the TMG. J R Colloid Surg Edinb 1982;27:209—18.
8. Verneuil E, Huanh CS, Chen YR. Temporomandibular joint reconstruction in children using costochondral graft. J Oral Maxillofac Surg 1999;57:789—98
9. Doss RB. Costochondral grafts replacing the mandibular condyle. Cleft Plate Craniofac J 1999;36:334—9.
10. Gett SA. Tempromandibular joint ankylosis the rationale for grafting in the young patients. J Oral Surg 1973;31: 744—8.
11. Agqvist C, Autogenous costochondral graft in temporomandibular joint arthroplasty.. J Maxillofac Surg 1986;14:143—9.
12. Suyuron B, Lasa CI. Unpredictable growth pattern of costochondral` graft. Plast Reconstr Surg 1992;90:880—5.
13. Saarx RE. The science and art of reconstructing the jaws and temporomandibular joints. In: Bell WH, editor. Philadelphia: Saunders; 1992. p. 1448—1531.
14. El-Sheikh MM, Medra AM, Warda MH. Bird face deformity secondary to bilateral temporomandibular joint ankylosis J Craniomaxillofac Surg 1996;24-96:101.
15. El-Sheikh MM, Medra AM. Management of unilateral temporomandibular joint ankylosis associated with facial asymmetry. J Craniofac Surg 1997;25:1—7.
16. Al-Kayat A, Bramley P. A modified pre-auricular approach to the temporomandibular joint and malar arch. Br J Oral Surg 1979; 17:91—103.
17. Svensson B, Adell R. Costochondral grafts to replace mandibular condyles in juvenile chronic arthritis patients:. J Craniomaxillofac Surg 1998;26:275—285.
18. Lindqvist C,. Adaptation of autogenous costochondral graft used for temporomandibular reconstruction. J Oral Maxillofac Surg 1988;46:465—470.
19. Peltomaki T, Ronning O. Interrelationship between size and tissue-separating potentials of costochondral transplants. Eur J Orthod 1991;13:459—465.
20. Kabban LB, Mulliken JB, Murray JE. A protocol for management of temporomandibular joint ankylosis. J MaxillofacSurg 1990;48:1145—1151
This article licensed under the Creative Commons Attribution 4.0 International License CC-BY 4.0., which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are properly credited.