
NL Journal of Dentistry and Oral Sciences
(ISSN: 3049-1053)
Unraveling the Enigma of Odontome: A Spectacular Case Report
Author(s) : Blessy, Eshna Sharma, Harman Chahal, Navneet Kaur, Megha Bahal, Avishi Syal. DOI : 10.71168/NDO.01.01.103
Abstract
This is a case report of clinical case reported at oral medicine depart of symptomatic odontome in the posterior upper and lower right region. Cone beam computed tomography (CBCT) was performed for precised 3-D imaging. The treatment protocol includes surgical enucleation of odontome and super numery tooth.
Introduction

A 32 year old female patient reported to the department of oral medicine and radiology with chief complain of pain in lower and upper right back tooth region of jaw from last 10 days. Pain reported is sharp, continuous, radiating towards head and aggravated on mastication patient reported with no past medical history. Diet of patient is mixed, and she brushes once daily with a toothbrush and manjan. On intraoral examination the area #46, #26 were tender on percussion with overhanging filling was observed at the same region. There was a bulge observed at #46 region which was tender on the percussion CBCT was advised to the patient.

a, b) Patient front view and lateral view with no swelling
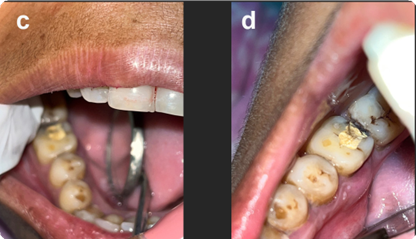
c,d ) Intraoral images showing buldge at #46 region
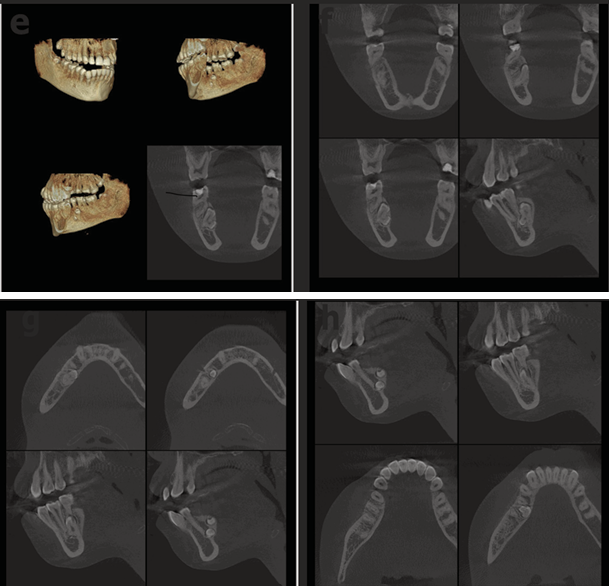
e,f,g,h) Coronal cone beam tomography scans revealing impacted supernumery tooth and odontoma present adjacent to the lingual cortex
Final diagnosis after CBCT
- Restored tooth relation to 46 with overhanging
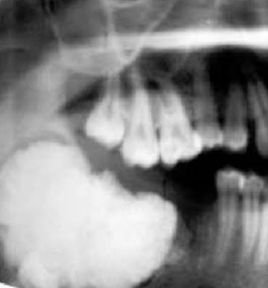
- Irregular radiopacity present in inter radicular region of 46 and 45 mimicking tooth structure suggestive of odontoma
- Evaluation of Odontoma:
- Odontome present adjacent to lingual
- Lingual cortical plate resorbed for the eruption of
- Roots of 46 adjacent to the crown of
- Roots of the 46 not resorbed and present buccal to the
- Odontome has bifurcated crown suggestive of geminated tooth
- Round peri coronal radiolucency present with distinct borders suggestive of dilated follicular
- Bifurcated crown of the odontome present occlusally and horizontally to the periapical region of
- Distance of the bifurcated horizontal crown from the apex of 45 is 68 mm.
- Distance of the odontome from the anterior loop of the mandibular canal is 6 mm.
- The [1] fused root of the odontome overlaps the inferior alveolar canal causing discontinuity of the inferior alveolar nerve vigilant extraction recommended of the odontome.
Discussion
Odontomas are the [1] developmental malformation of the dental tissues. They are hamartomas also commonly known as odontome. They have all the basic histological structures of a tooth but in a disoriented fashion or may differ morphologically. They are odontogenic in origin and generally found between 10-20 years old. Most common site are [3] anterior maxilla and mandible [4] Odontomas can be classified as [4] Compound and Complex Odontomas
Compound odontoma
4.Probably produced by [6] localized multiple budding off from the dental lamina and formation of many tooth germs
5.Consists of many separate, small tooth like structures
6. Gives rise to a painless swelling in the anterior part of the jaws clinically.
7. Radiographically [3] seen as separated densely calcified tissue.
8.Histologically, the denticles are embedded in [2] fibrous connective tissue having a fibrous capsule

Complex odontoma
9. Irregular mass of hard and soft dental tissue showing no resemblance to a tooth
10. Clinically hard [7] painless swelling seen in young persons
11. Radiographically seen as a [1] radiopaque irregular mass when fully calcified with areas of densely radiopaque enamel.
12. Histologically, tissues arranged in a disordered arrangement frequently in a radial pattern
13. Multiple [6] branching of pulp gives a sponge like appearance
Management
The mass of tissues are generally removed by [7] conservative method but in this clinical case it should be removed aggressive because it is located near to the inferior alveolar nerve. They generally respond to enucleation.
Conclusion
Odontomas are typically characterized by benign and asymptomatic lesions that may lead to disturbances in the eruption of teeth, such as delayed eruption of primary or permanent teeth or retention of primary teeth. The majority of patients are diagnosed with odontoma during a routine radiographic examination. While an odontoma is a tumor, it’s a benign one and not uncommon. That alone is great news! However, odontomas usually require surgical removal. They’re made up of dental tissue that resembles abnormal teeth or calcified mass that invade the jaw around your teeth and could affect how your teeth develop. Conventional surgery is considered to be the treatment of choice for odontomas. The WHO classifies odontomas as benign mixed odontogenic tumors. Given their behavior, they are considered hamartomatous lesions arising from dental tissues.
References
1. Cawson RA,Binnie WH,Barrete AW,Speight P,Wright JM 1998 Lucas’s pathology of tumors of the the oral tissues.Churchill livingston, Edinburgh.
2. Jonquiere L, de Vicente JC, Roig P, Olay S, Rodrí�guez-Recio O (2005)
3. “Intraosseous odontoma erupted into the oral cavity: an unusual pathology”. Med Oral Patol Oral Cir Buca/10 (3):248-51. PMID 15876969.
4. Oral Pathology Glossary O”. Retrieved 2009-01-04
5. “Odontogenic tumors”. Retrieved 2009-01-04. da Costa CT, Torriani DD, Torriani MA, da Silva RB (2008).“Central incisor impacted by an odontoma”. J Contemp Dent Pract 9 (6): 122
6. PMID 18784868.A Amado Cuesta S, Gargallo Albiol J, Berini Aytés L, Gay Escoda C (2003).
7. Review of 61 cases of odontoma. Presentation of an erupted complex odontoma”. Med Oral 8 (5): 366-73.PMID 14595262.
This article licensed under the Creative Commons Attribution 4.0 International License CC-BY 4.0., which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are properly credited.