
NL Journal of Dentistry and Oral Sciences
(ISSN: 3049-1053)
Effect of Subgingival Application of Ozonated Olive Oil Versus Olive Oil as an Adjunct to Scaling and Root Planing in Chronic Periodontitis: A Clinical and Microbiological Study
Author(s) : Navneet Kaur, Bhavya Pruthi, Gurpreet Kaur. DOI : 10.71168/NDO.01.01.102
Abstract
Introduction: Periodontitis is an infectious disease that results in inflammation and destruction of the periodontal tissue. The primary goal of periodontal treatment is the elimination or reduction in the number of pathogenic bacteria. SRP does not completely eliminate the residual pockets and periodontopathogenic bacteria. Ozone is a competitive antimicrobial agent effective against Gram-Positive and Gram-Negative bacteria, fungi, protozoa and viruses. The application of Ozonated olive oil reduces plaque and gingival score and reduces the colony count of streptococcus mutans and lactobacillus. Therefore, the present study was conducted to compare and evaluate the clinical and microbiological outcomes of ozonated olive oil and olive oil as an adjunct to scaling and root planning. Aim & Objective: To compare the clinical and microbiological effect of the subgingival application of ozonated olive oil versus olive oil as an adjunct to scaling and root planning (SRP) in chronic periodontitis. Materials and Methods: A total of 6 patients within the age group of 20-50 years with probing pocket depth 4-7mm were randomly selected and divided into 2 groups: Group 1- 3 Patients were treated with scaling and root planning (SRP) with Olive Oil. Group 2- 3 Patients were treated with scaling and root planning (SRP) with Ozonated Olive Oil. All the patients were evaluated for clinical parameters such as Plaque Index, Gingival Index, Probing Pocket Depth and anaerobic microbial analysis at baseline and after 1 month. Results: The result showed an improvement in all clinical parameters such as PI, GI and PPD in both study groups when measured at baseline and after 1 month. The microbiological analysis showed a reduction in Colony Forming Units for anaerobic micro flora as compared to group 2 and group 1. However, the microbiological assessment was found to be statistically non-significant (p>0.05). Conclusion: Based on the result of the study it can be concluded that subgingival application of ozonated olive oil could be a promising adjunctive measure and provide an additional benefit in terms of clinical and microbiological parameters. However, long term studies with large sample size are required to evaluate the efficacy of ozonated olive oil. keywords: Chronic Periodontitis, Ozonated Olive Oil, Ozone therapy, Olive oil, Subgingival application.
Introduction
Periodontitis is a destructive inflammatory disease of supporting tissues of teeth which is multifactorial in origin resulting in the pocket formation, gingival recession and destruction of supporting periodontal attachment apparatus. The initiation and progression of periodontitis is due to dental plaque along with anerobic periodontal pathogens that are adhere to both hard and soft tissues. The primary goal of periodontal therapy is to eliminate the number of pathogenic microbiota that are responsible for the causation of inflammatory response.
The most common periodontal pathogens ass are Porphyromonas gingivalis, Treponema denticola, Tannerella forsythia, Prevotella intermedia, Campylobacter rectus, Aggregatibacter actinomycetemcomitans. These periodontal pathogens usually present sub-gingivally into the deeper segment of periodontal pocket during the disease activity which is called Period of Exacerbation [1]. With the progression of time these periodontal pathogens become more pathogenic in action resulting in eventually the bone destruction because of the release of the endotoxins from periodontal pathogens itself. The periodontal pathogens present in the biofilm are well protected from host immunological mechanism as well as from chemotherapeutic agents used during the treatment therefore it is necessary to treat the periodontal pocket through mechanical debridement of primary etiological and iatrogenic factors resulting in destruction of subgingival plaque itself.
The professional Phase I Therapy includes removal of plaque through scaling and root planning procedures which is considered as Gold Standard among non-surgical treatment modalities in Chronic Periodontitis [2]. The mechanical plaque control is achieved both professionally and by the patient at home. Various mechanical oral hygiene measure includes tooth brushing, interdental cleaning aids and subgingival irrigation performed by patient at home. The complex anatomy of root, root concavities, furcation involvement and deep periodontal pockets may alter the treatment and prevent the sufficient reduction of bacterial load also the effectiveness of Phase I Therapy along with endotoxins penetrating deeper into the subgingival tissues may decreases and may start recolonization within 60 days after SRP [3,4,5].
Hence there is a need of alternative to conventional antimicrobial or antiseptic agents which may result in suppression of subgingival bacteria by changing the subgingival environment and has been shown to be highly effective against anaerobic pathogens with a prevailing low oxygen tension [6]. The repeated subgingival application of oxygen into the deeper periodontal pockets have shown a significant improvement in all the clinical parameters of periodontal condition. There are various methods for altering the subgingival environment which includes the application of oxygenating and redox agents [7]. These agents have been applied as a molecular oxygen, hyperbaric oxygenation and hydrogen peroxide. Recently, Ozone therapy is gaining popularity in various treatment modalities and is also being successfully utilized in any form (gaseous, water, oil) for the management of dental diseases such as dental caries, periodontitis and hypersensitivity. Ozone has been shown to be detrimental against bacteria, fungi, viruses and protozoa in vitro.
Ozone is a chemical compound consists of 3 oxygen atoms (O3- triatomic atom) and have a triangular configuration. Naturally, it is present as a gas with a pale blue color and pungent odor having reminiscent of chlorine. It is available and administered in 3 forms- gaseous, water and oil. Ozone exerts its antimicrobial action through its synergistic effect resulting in damaging of cytoplasmic membrane because of ozonolysis and ozone induced modification of intracellular contents because of secondary oxidant effects. The other biological action of ozone is immunostimulant effect, biosynthetic effect (activation of metabolism of carbohydrates, proteins, lipids anti- hypoxic effect, analgesic, hemostatic and bioenergetic. It does not damage healthy human body cells because they have free radical scavengers like superoxide dismutase, catalase, hydrolase and antioxidants like vitamin C, E and beta carotene which further inhibit the uncontrolled activity of free radicals and protect the healthy cells. Ozonated olive oil is found to be efficacious against streptococci, enterococci, pseudomonas, staphylococcus, E coli and specially myco-bacteria and also useful to cure fungal infections [8].
Ozone has the capability to improve the circulatory system and modify the immune response which make it as a therapeutic agent of choice for treatment of pathologies and various infectious oral diseases. Ozone is a non-inva- sive minimal intervention technique and an oxidizing effect on periodontal tissues. Moreover, it has high level of biocompatibility to fibroblasts, cementoblasts and epithelial cells suggesting its effectiveness. The data available in the literature both clinical and microbiologically is very scant. Hence in the light of the above facts, the present was conducted to compare and evaluate the clinical and microbiological effect of the subgingival application of ozonated olive oil versus olive oil as an adjunct to scaling and root planning (SRP) in chronic periodontitis.
Materials and Methods
Study Population
For the proposed study, a total of 6 patients will be selected from the outpatient department of Periodontics and Oral Implantology. This pilot study was done in the Department of Periodontology and Oral Implantology, National Dental College & Hospital, Derabassi, Punjab. An ethical approval for the study was obtained from the Institutional Ethical Board Committee and a detailed verbal and written consent was taken from each of the patient. Randomized control clinical trial were performed. Patients were allocated randomly into two study groups (3 in each group) Group 1- Scaling and root planning (SRP) + Subgingival application of olive oil and Group 2- Scaling and root planning (SRP) + Subgingival application of Ozonated olive oil .
Inclusion Criteria:
- Patients between the age group of 20-50
- Probing pocket depth of 4-7mm which is not associated with
- Absence of any systemic
Exclusion Criteria:
- Pregnant or lactating
- Patients suffering from known systemic
- Any surgical or non- surgical therapy 6 months before the start of the
- Antibiotic therapy in last 6
- Chemotherapeutic mouth rinses past 6
- Habits- smoking, tobacco and pan
- Pockets with recession.
Methodology
All patients were underwent a full mouth scaling using ultrasonic scalers and hand instrumentation. Depending on the group, patient received subgingival application of oils in the deepest selected periodontal pocket using a disposable 5-ml plastic syringe with a needle of 24 gauge and of 0.55 diameter bend at the tip.
The selected teeth were thoroughly dried with cotton rolls, and then, oil was applied carefully subgingivally and interproximally, until excess oil is observed from the gingival margin. This procedure was repeated for all teeth to be treated. The excess oil was removed with a cotton roll. Oil application was performed after initial SRP and at 7, 14 and 21 days. The reinforcement of oral hygiene instructions was done at each appointment.
Subgingival Plaque samples was taken on the initial day and after 1 month of the treatment. The supragingival plaque was removed with a sterile curette and cotton gauze. Subsequently, a subgingival plaque sample was obtained using one sterile paper points, inserted into the pocket until resistance was met or the paper points bent. It was kept in place for 10 s and then transferred to 10 ml thioglycolate broth. This test tube was kept in an incubator for 24 h. Blood agar plates were used to conduct the microbial analysis. Blood agar was used because it is a general purpose, nonselective, and enriched medium that promotes the growth of the microorganism. Anaerobic microbial analysis was performed. Ozone oil used was commercially available at the Ozone Forum of India.
Assessment of Clinical and Microbiological Parameter
Clinical parameters included the assessment of probing pocket depth (PPD) using UNC-15 Periodontal probe, Plaque index(PI) Silness & Loe (1964). Gingival index (GI) Loe & Silness (1963) measured at baseline and 1 month.
For microbiological assessment Colony Forming Units were counted. Bacterial count (Colony forming unit- cfu/ml)
 Statistical Analysis
Statistical Analysis
The parameters were tabulated and put to statistical analysis. The data for the present study was entered in the Microsoft Excel 2007 and analyzed using the SPSS statistical software 23.0 Version. The descriptive statistics included mean, standard deviation frequency and percentage. The intragroup comparison for the different time intervals was done using Paired t-tests to find the difference between the individual time intervals. The level of the significance for the present study was fixed at 5%. The intergroup comparison for the difference of mean scores between independent groups was done using the one way ANOVA and Post Hoc Tukey Analysis.
Results
Table 1: Comparison of all clinical parameters at various time interval.
| PLAQUE INDEX
(Mean ± SD) |
GINGIVAL INDEX
(Mean ± SD) |
PROBING POCKET DEPTH (Mean ± SD) | ||||
| Group 1 | Group 2 | Group 1 | Group 2 | Group 1 | Group 2 | |
| BASELINE | 2.00±00 | 1.76±0.25 | 2.00±0.00 | 1.96±0.35 | 5.00±0.00 | 4.66±0.57 |
| DAY 30 | 1.70±0.00 | 1.63±0.20 | 1.63±0.05 | 1.53±0.35 | 4.33±0.57 | 3.66±0.57 |
| P value | NC | 0.27 | 0.008* | 0.166 | 0.184 | NC |
*P value <0.05 (statistically significant)
*P value >0.05 (non-statistically significant)
NC- not calculated because no deviation in the data set i.e. SD is zero.
The intragroup comparison of the plaque Index and probing pocket depth between the time intervals i.e. at Baseline and 30th day was statistically non-significant for both groups i.e. Group 1 (olive oil and SRP) and Group 2 (Ozonated Olive Oil and SRP). However. Gingival Index was statistically significant in Group 1 (Olive oil and SRP) between the time intervals i.e. baseline and 30th day.
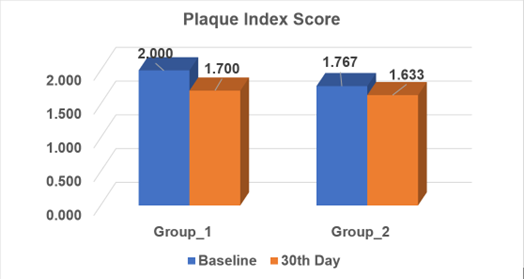
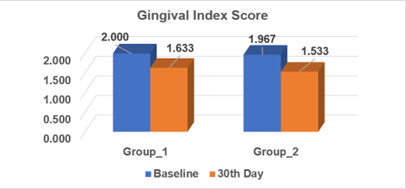
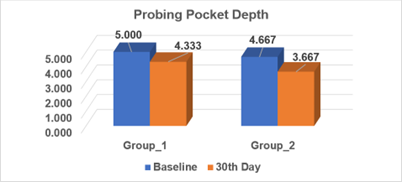
Table 2: Comparison of microbiological parameters at various time intervals.
| COLONY FORMING UNITS (×102)
(Mean ± SD) |
||
| Group 1 | Group 2 | |
| BASELINE | 41.61±38.48 | 37.33±30.92 |
| DAY 30 | 15.80±17.54 | 5.13±5.70 |
| P value | 0.177 | 0.166 |
*P value <0.05 (statistically significant)
*P value >0.05 (non-statistically significant)
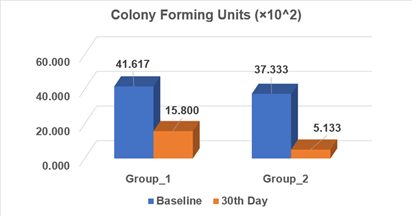
The intragroup comparison of the colony forming units between the time intervals at Baseline and 30th day was statistically non-significant for both the groups i.e. Group 1 (olive oil and SRP) and Group 2 (Ozonated Olive Oil and SRP).
Discussion
Both dental caries and periodontal disease are one of the most common forms of microbial diseases and has significantly affect the systemic health and quality of life of an individual [9]. The oral cavity serves as a focal point of entry for periodontal pathogens and enter into the systemic circulation also the lack of oral hygiene may increase the number of virulent periodontal pathogens in the oral biofilm. Therefore, both mechanical and chemical means of plaque control is important to prevent gingivitis and periodontal diseases. Various forms of alternative or traditional treatment are available in the form of antibiotics and antiseptics which are used locally as an adjunct to mechanical therapy. Several antimicrobial chemotherapeutic agents which may vary in concentration and formulations has been used. Several local drug delivery devices have become commercially available which are used in dentistry. Currently, ozone therapy is gaining popularity as a modern non-invasive method of treatment. When ozonoid reaction may occurs, it can induce disruption of microbial cell wall [10].
A new ozonated olive oil is now available in the field of dentistry as an alternative to Chlorhexidine with lower side effects. Ozonated olive oil is basically produced through chemical reaction between ozone and olive oil. When ozone activates the oxygen molecule, it is funneled into a tube and an electrical charge is generated. During this process, ozone is slowly infused into olive oil and ozonated olive oil is created. For the physiochemical property there is a chemical reaction called ozonolysis between ozone and unsaturated fatty acid of olive oil especially alkaline in the fatty acid [11]. Regarding the safety of ozone as an alternative antiseptic, the aqueous form of ozone proved highest level of biocompatibility on oral epithelial cells, gingival fibroblasts and periodontal cells [12,13]. Hence, the present study was planned to compare and evaluate the clinical and microbiological effect of the subgingival application of ozonated olive oil versus olive oil as an adjunct to scaling and root planning (SRP) chronic periodontitis.
In the present study ozonated olive oil was selected because oil was found to provide a long stay in oral cavity and higher efficacy. When the gaseous form of ozone is dissolved in an oil base, it chemically reacts with oil and form a long complex molecule [14]. Ozonated olive oil can be an effective ozonated therapy against plaque induced gingivitis when an ozone molecule dissociates into oxygen it may create an oxygen rich environment thus, disturbing the normal ecosystem of plaque. Montevecchi et al 2013 found that ozonated olive oil is more effective antiseptic as compare to CHX and Povidone iodine against Streptococcus aureus and P. gingivalis [15]. The enzymatic control system of bacterial cell is blocked because ozone may inhibit the glycoproteins, glycolipids and other amino acids resulting in functional cessation and death of microorganisms.
In the present study the subgingival application of ozonated oil is done at baseline, 7th day, 14th day and 21st day after the intervention. The evaluation in this study included both clinical and microbiological assessment. Clinical assessment was based on plaque index, gingival index and probing pocket depth were recorded at baseline and after 30th day. There was a significant reduction in plaque index in between two groups from baseline to 30th day. However, it was found to be statistically non significant when compared on inter and intragroup comparision. The reduction in plaque might be due to the viscosity of oil or spoanification of the process resulting in hydrolysis of fat. The results of the study were in accordance with various studies who investigated for ozone therapy in periodontitis. Durga K. et al 2010 also found the similar reduction in GI and PI. The reduction in mean PI was 0.16 ± 0.33, GI 0.34 ± 0.38, which was similar to our study in which we found reduction of PI 1.70±0.00 in group 1 and PI 1.63±0.20 in group 2 after 30th day of intervention. Verma et al in 2016 compared the effects of ozonated olive oil with CHX gel and concluded that there was a significant reduction in plaque index in both the groups [16].
There was also significant reduction in gingival index in between 2 groups GI was 1.63± 0.05 in group 1 and 1.53±0.35 in group 2 after 30th day of intervention. However, the results was found to be statistically non significant when compared on inter and intra group comparision. Similarly, K Dhingra 2011 and conducted a study in orthodontic patients having gingival inflammation and concluded that ozonated olive oil is effective in reduction and improvement in all the clinical parameters [17]. Also, Francesco Carinci conducted a clinical and micobiological study in 2015 with the same clinical results and showed an improvement in clinical parameters and reduction in the count of T forsythia pathogen when compared to SRP alone and was found to be significant [18] In the present study a significant reduction was found in PPD on 30th day from the baseline in the ozonated olive oil group as compared to olive oil group. Similar study was conducted by Katti and Chawa in 2013 and Ciancia et al in 1989 and concluded that antimicrobial agents has a beneficial effect on the oral health status . The ozone molecule involved in a direct reactions of molecular ozone and result in generation of free radical which cause destruction to the supporting tissues [19].
Microbiological parameter was also seen as Colony Forming Units in group 1 and group 2 from baseline to 30th day. There was a significant reduction in the Colony Forming Units from baseline to 30th day. However there was no statistical significant difference is seen in both the groups. Similarly a microbiological parameter which is accordance with the study by Vandana et al 2014.The subgingival application of ozonated olive oil along with SRP significantly reduces the anaerobic bacterial count in periodontal pocket and also prevent their recolonisation. Ahu Uraz in 2018 published a study to evaluate the effect of ozone therapy on microbiological parameter which ws analyzed by quantitative PCR and GCF biomarkers were assessed by ELISA and revealed that there was a significant reduction in periodontal pathogens such a P.gingivalis, T.forsythia and P.intermedia level in both test and control group but no statistically significance was noted during intergroup comparision [20].
There were many studies in the literature who supported for the use of ozonated olive oil as an adjunct to SRP in chronic periodontitis cases although in the literature there were some studies who did not get any positive result or significant improvement in terms of clinical parameters while using ozone as an adjunct to SRP. Muller P. 2007 and Eltas SD et al 2019 Zekeriya T et al 2019 did not yield any significant reduction in clinical as well as microbiological parameters when ozone used as an adjunct to SRP [21]. The reason might be due to inability of the patient for compliance and follow up of the oral hygiene instructions along with time period of intervention for scaling and root planning for which the patients are included through inclusion criteria.
Within the limitation of study in terms of very short sample size and limited follow up time period that is 1 month is the major and important limitation to reach at significant conclusion. Since this study has shown a positive result in terms of clinical and microbiological parameter but statistically there was no significant difference in between the groups. To prove the significance and positive outcome when ozonated olive oil used as an adjunct to SRP further research can be carried out on large sample size.
Conclusion
Ozone therapy is one of the non-invasive methods which increases patient acceptability and compliance with minimal adverse effects. Based on the results, the present study indicates that the adjunctive use of ozonated olive oil after scaling and root planning improved the treatment outcome in subjects with chronic periodontitis. Ozone is an antiseptic antimicrobial agent which can be used safely in the treatment of moderate to deep periodontal pockets. Further studies need to be conducted with larger sample size, different concentrations and a greater number of subgingival applications with follow up time period of ozonated olive oil. Also, biochemical parameters to assess GCF biomarkers are needed to be investigated with use of ozonated olive oil in chronic periodontitis.
References
- Haffajee, AD, Cugini,MA, Dibart,S,Smith, C, Kent, RL &Socransky, SS 1997, ‘The effect of SRP on the clinical and microbiological parameters of periodontal diseases,’ Clin. Periodontol., vol. 24, no.5, pp. 324-334.
- Cobb, CM 2008, ’Microbes, Inflammation,Scaling and Root Planing, and the periodontal condition,’ Dent. Hyg, vol. 82, no. 2, pp. 4-9.
- Stabholz, A, Sela, MN, Friedman, M,Golomb, G & Soskolne,A 1986, ‘Clinical and Microbiological effects of sustained release of chlorhexidine in periodontal pocket’, Clin. Periodontol , vol. 13, no. 8, pp. 783-788.
- Mandel, ID 1988, ‘Chemotherapeutic agents for controlling plaque and gingivitis,’ Clin. Periodontol, vol. 15, no. 8, pp. 488-498.
- Donald, A 1998, ‘Nonsurgical Pocket Therapy: Mechanical, Pharmacotherapeutics and Dental Occlusion,’ J Am Dent Assoc, 129, pp. 34s-39s.
- Mettraux GR, Gusberti FA, Graf H 1984,’ Oxygen tension (pO2) in untreated human periodontal pockets’, Clin. Periodontol, vol. 55, pp. 516-521.
- Marsh, PD,1994, ‘Microbial ecology of dental plaque and its significance in heath and disease’, J Am Dent Assoc , 8, pp. 263- 271.
- Gupta, S, and Deepa, D, 2016,’ Applications of ozone therapy in dentistry,’Jornal of Oral research and review, 8, no.2, pp. 86.
- Segata N, Haake SK, Mannon P, Lemon KP, Waldron L, Gevers D, et al 2012, ‘Composition of the adult digestive tract bacterial microbiome based on seven mouth surfaces, tonsils, throat and stool samples’, Genome Biol, 13, pp. 42.
- Shapiro S,1996, ‘The inhibitory action of fatty acids on oral bacteria’, Oral Microbiol Immunol, 11, no. 5, pp. 350-5.
- Patel PV, Kumar S, Vidya GD, Patel A, Holmes JC, Kumar V, 2012, ‘Cytological assessments of healing palatal donor site wounds and grafted gingival wounds after application of ozonated oil: An eighteen-month randomized controlled clinical trial’, Acta Cyto, 56, no.3,pp. 277-84.
- Huth KC, Jakob FM, Saugel B, Cappello C, Paschos E, Hollweck R, Hickel R, Brand K, 2006, ‘Effect of ozone on oral cells compared with established antimicrobials’, Eur J Oral Oct, vol.114, no.5, pp.435-50.
- Azarpazhooh A, Limeback H, 2008, ‘The application of ozone in dentistry: A systematic review of literature’, J Dent, vol.36, 2,pp. 104-16.
- Cruz O, Menedez S, Martinez ME, Clavera T, 1997, ‘Application of ozonized oil in the treatment of alveolitis’ 2nd International Symposium on Ozone Applications Havana, Cuba 24-26.
- Montevecchi M, Dorigo A, Cricca M, Checchi L 2013, ‘Comparison of the antibacterial activity of an ozonated oil with chlorhexidine digluconate and povidone-iodine. A disk diffusion test’, New Microbiologic, 36, pp.289-302.
- Verma SK, Deo B, Ranjan M, Prakash O, Shekhar M, Verma S,2016, ‘Comparision of efficacy of ozonated oil and chlohexidine gel in the management of gingivitis’, Int J Curr Res, 8, no.3, pp.76-9.
- Dhingra K, Vandana KL,2011, ‘Management of gingival inflammation in orthodontic patients with ozonated water irrigation- a pilot study’, Int J Dent Hygiene, 9, pp. 296-302.
- Carinci F,Palmeri A,Girardi A, Aqolab, 2015, ‘ozone therapy in an efficient adjunct in treatment of chronic periodontitis: A case– control study’, J of Orofacial Sci, vol. 7, pp. 27-32.
- Katti SS, Chava VK, 2013, ‘Effect of ozonized water on Chronic Periodontitis – A Clinical Study’, J Int Oral Health, 5, pp. 79-84.
- Uraz A, Karaduman B, Isler SC, Gonen S, Cetiner D, 2018, ‘Ozone application as adjunctive therapy in chronic periodontitis: Clinical, microbiological and biochemical aspects’ , Journal of Dental Sciences,vol. 06, 05.
- Muller, B.Guggenheim, P.R Schmidlin, 2007, ‘Efficacy of gasiform ozone and photodynamic therapy on a multispecies oral biofilm in vitro’, Eur J Oral Sci, vol. 115, pp. 77-80.
This article licensed under the Creative Commons Attribution 4.0 International License CC-BY 4.0., which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are properly credited.