
NL Journal of Dentistry and Oral Sciences
(ISSN: 3049-1053)
Healing Large Periapical Lesions Using Metapex—Report of a Case Series
Author(s) : Nandita Mohan, Satendra Singh. DOI : 10.71168/NDO.02.05.131
Abstract
Objective: To evaluate the clinical and radiographic effectiveness of Metapex as an intracanal medicament in the nonsurgical management of large periapical lesions. Methods: Three female patients (ages 44-55) presented to the Dental Department of Sanjeevan Hospital, Delhi, with extensive periapical radiolucencies associated with teeth 15, 26 and 46. Each case underwent thorough chemo mechanical debridement followed by placement of Metapex, a silicone-oil-based paste containing calcium hydroxide, 38% iodoform, and barium sulfate into the prepared canals. Systemic antibiotics were prescribed initially. Metapex dressings were refreshed at regular intervals over a period of four to five months. Patients were assessed for pain, swelling, and inter-appointment discomfort, and radiographic healing was monitored at 3-week, 2.5-month, and 5-month follow-ups. Results: All three patients reported complete resolution of pain and soft-tissue swelling without any inter- appointment discomfort. Serial periapical radiographs demonstrated progressive reduction in lesion size, with full trabecular bone regeneration observed by 2.5 months in the first case and by five months in the remaining cases. No adverse reactions or procedural complications were noted. Conclusion: Metapex, used as an intracanal dressing following conventional root canal therapy, facilitated predictable healing of large periapical lesions in this case series. Its combined antimicrobial action, biocompatibility, and radiopacity support its role as a first-line adjunct in conservative endodontic protocols for extensive periapical pathology. Keywords: Metapex, Intracanal medicament, Periapical lesion, Non-surgical endodontic treatment, Calcium hydroxide.
Introduction
Periapical abscesses, often resulting from untreated pulp infections, pose a significant challenge in endodontic practice due to their potential to cause pain, swelling, and bone destruction. The necrotic dental pulp occurs as a consequence of dental caries, operative dental procedures and trauma and consists of a biofilm which is mostly anaerobic bacterial flora [1]. These can cause pulpal necrosis often which stimulate an immune response in the periapical region leading to a periapical lesion. Periapical lesions can promote the development of dentoalveolar abscess and periapical bone loss. They are generally diagnosed either during dental radiographic examination or following acute pain in tooth. The periapical lesions are mostly classified as periapical cyst or granuloma or abscess [2].
While conventional root canal therapy remains the cornerstone of treatment, complete disinfection of the root canal system is not always achievable through instrumentation and irrigation alone. The main goal of root canal therapy is to eliminate the microbial growth emerging through the apical foramen and prevent its further spread [3]. The primary aim of any treatment should be a painless and conservative approach [4]. This is where intracanal medicaments play a vital role.
Based on conservative endodontic treatment there are various intracanal medicaments like calcium hydroxide, antibiotics, steroids, etc for the management of periapical abscess whereas calcium hydroxide based intracanal medicaments are considered as the gold standard mainly because of its high alkalinity tissue dissolving effect, causes induction of repair by hard tissue formation and bactericidal effect.
To improve the properties of calcium hydroxide, the mixture of other substances ae usually added. These substances can be vehicles that can speed up ionic dissociation, substances that aid the filling of pulpal cavity due to their consistency, substances used as antimicrobial medium and media that enhance radiopacity. Metapex, a combination of calcium hydroxide and 38% iodoform using silicone oil as base is very popular [5].
Metapex, a paste composed of calcium hydroxide, iodoform, and barium sulfate has its advantages- its potent antibacterial properties, biocompatibility, and ability to promote periapical healing make it a valuable adjunct in non-surgical endodontic therapy. Clinical case reports have demonstrated remarkable healing of large periapical lesions following Metapex application, highlighting its efficacy in controlled sepsis and microbial suppression.
This article comprises a series of cases reported to the Dental Department of Sanjeevan Hospital, Delhi with periapical lesions that were nonsurgically managed by placement of Metapex in the root canals.
Case Reports
Case 1
A 44-year-old woman presented to our dental department in May 2025 with a one-week history of a prominent left facial swelling extending from the corner of her mouth to the lower border of her left eyelid, accompanied by restricted eye opening. Her dental history was notable for a large amalgam restoration on tooth 26. Periapical radiography revealed an extensive radiolucent lesion associated with the palatal root of that tooth.
An immediate root canal treatment was initiated. Upon removing the restoration, a foul-smelling cotton pellet was discovered beneath it, and instrumentation of the palatal canal yielded purulent discharge. The mesiobuccal and distobuccal canals exhibited apical calcifications but were successfully negotiated. After several sessions of open dressing, Metapex was placed as the intracanal medicament, and the patient was started on systemic antibiotics.
Three weeks post-treatment, the facial swelling had markedly diminished. Follow-up radiographs demonstrated progressive lesion regression, and at 2.5 months the periapical defect was largely replaced by healthy trabecular bone.
 Figure 1: Pre operative IOPA revealing a huge periapical lesion wrt palatal root of 26.
Figure 1: Pre operative IOPA revealing a huge periapical lesion wrt palatal root of 26.
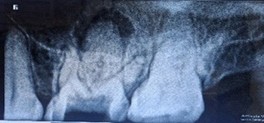 Figure 2: Immediate post-op after removing faulty restoration and access opening initiation.
Figure 2: Immediate post-op after removing faulty restoration and access opening initiation. Figure 3: Three weeks post op Xray after metapex placement revealing no marked changes in the periapical lesion.
Figure 3: Three weeks post op Xray after metapex placement revealing no marked changes in the periapical lesion.
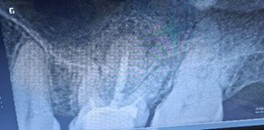 Figure 4: Two and half months post op Xray after metapex placement reveals nearly complete resolution of periapical radiolucency.
Figure 4: Two and half months post op Xray after metapex placement reveals nearly complete resolution of periapical radiolucency.
Case 2
A 51-year-old woman presented with a 15-day history of persistent pain in the right mandibular posterior region. Her dental record showed multiple failed restoration attempts and an incomplete root canal on tooth 46, yet her symptoms persisted. Clinical examination and intraoral periapical radiography revealed furcation involvement, a large periapical radiolucency, and a perforation in the pulp chamber floor.
Despite a guarded prognosis for tooth survival, we performed thorough canal disinfection and placed Metapex as an intracanal medicament for four weeks. The patient reported no inter-appointment discomfort. At the subsequent visit, radiographs confirmed complete resolution of the periapical lesion, and root canal obturation was successfully completed.
 Figure 1: Pre operative IOPA wrt 46 showing incomplete root canal treatment, with furcation involvement, a large periapical lesion and perforation of pulp chamber floor.
Figure 1: Pre operative IOPA wrt 46 showing incomplete root canal treatment, with furcation involvement, a large periapical lesion and perforation of pulp chamber floor. Figure 2: Metapex placement after thorough canal disinfection.
Figure 2: Metapex placement after thorough canal disinfection. Figure 3: Post 4 weeks, complete resolution of periapical lesion.
Figure 3: Post 4 weeks, complete resolution of periapical lesion. Figure 4: Post obturation IOPA after 4 weeks.
Figure 4: Post obturation IOPA after 4 weeks.
Case 3
A 55-year-old woman presented to our department with a ten-day history of unrelenting pain in the upper right posterior region. Her prior medications provided no relief. Clinical examination of tooth 15 revealed mild vestibular swelling beneath a metal-free crown. Periapical radiography confirmed a large radiolucent area consistent with a periapical abscess. An earlier attempt at access had been made, with canals negotiated and prepared, but treatment remained incomplete.
We immediately initiated root canal therapy. Once the gingival swelling subsided, Metapex was placed as an intracanal medicament. The patient experienced no inter-appointment discomfort, and serial radiographs over five months demonstrated complete resolution of the lesion with restoration of healthy periapical bone.
 Figure 1: Pre operative IOPA revealing incomplete root canal treatment with crown placement wrt 15.
Figure 1: Pre operative IOPA revealing incomplete root canal treatment with crown placement wrt 15. Figure 2: Root canal initiated through crown and metapex placed.
Figure 2: Root canal initiated through crown and metapex placed.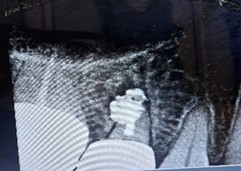 Figure 3: Post operative IOPA after 2 months reveals marked reduction in the lesion.
Figure 3: Post operative IOPA after 2 months reveals marked reduction in the lesion.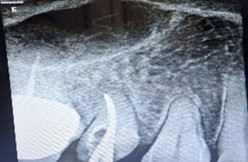 Figure 4: Post op IOPA after 5months reveals complete healing of periapical lesion, crown removal done, root canal master cone IOPA confirms.
Figure 4: Post op IOPA after 5months reveals complete healing of periapical lesion, crown removal done, root canal master cone IOPA confirms. Figure 5: Post obturation IOPA.
Figure 5: Post obturation IOPA.
Discussion
The present case series highlights the efficacy of Metapex as an intracanal medicament in the non-surgical management of extensive periapical lesions. In all three patients, placement of Metapex following thorough chemomechanical debridement resulted in marked reduction of soft-tissue swelling, elimination of patient discomfort between appointments, and progressive radiographic healing over a period of two to five months. These outcomes underscore Metapex’s role in promoting periapical repair even in cases with challenging anatomical features or prior treatment failures.
It is apparent that its use beyond the apex intentionally or accidentally has been associated with the successful nonsurgical management of many cases of large periapical lesions [6].
A appropriate treatment varies with the presence, nature and extent of involvement of the diseases for management of periapical abscesses, recommended protocol is drainage and after one week the definitive treatment could be carried out [7]. Recent studies have shown, however, that intracanal application of certain medicaments prior to the completion of endodontic therapy may produce highly favorable results when followed by conventional therapy, even when the periapical area is very large [8].
The advantage of performing non-surgical endodontic treatment with large periapical radiolucency is that it causes less psychological trauma and adds more comfort to the patient. The large periapical lesion in these cases have completely resolved. The periapical tissues is said to have the regenerative potential, so the treatment should always directed towards the removal of the causative factor alone [9].
Conclusion
Although it may be more time-consuming, a non-surgical approach should always be the initial choice before resorting to surgery. In this case, regular replacement of Metapex as an intracanal dressing, combined with thorough root canal therapy, proved highly effective in achieving complete healing of the periapical lesion.
References
1. G Sundqvist. Taxonomy, ecology, and pathogenicity of the root canal flora. Oral Surg Oral Med Oral Pathol 1994.
2. T Ishida. Pathology of periapical lesions. Oral Radiol 1998.
3. Choudhary D, Singh A, Wazir ND. Calcium hydroxide induced healing of periapical radiolucency: A case series. IP Indian Journal of Conservative and Endodontics. 2020 Sep 15;5(3):123-6.
4. Lin LM, Huang GTJ, Rosenberg PA. Proliferation of Epithelial Cell Rests, Formation of Apical Cysts, and Regression of Apical Cysts after Periapical Wound Healing. J Endod. 2007;33(8):908–16.
5. Gautam S, Rajkumar B, Landge SP. Antimicrobial efficacy of Metapex (Calcium hydroxide with Iodoform formulation) at different concentrations against selected microorganisms-An in vitro study.Nepal Med Coll J 2011;13(4):297-300.
6. Webber RT (1983) Traumatic injuries and the expanded endodontic role of calcium hydroxide. In:Gerstein CH, ed. Techniques in Clinical Endodontics. Philadelphia, PA: WB Saunders, pp.238–9.
7. Fernandes M, Ataide D. I. Nonsurgical management of periapical lesions. J Conserv Dent.2010;13(4):240-5.
8. Oztan, M.D. Endodontic treatment of teeth associated with a large periapical lesion, Int Endo J Jan 200235:1 pages73-78.
9. Ayodhi et al. IP Indian Journal of Conservative and Endodontics 2022;7(4):186–189.
This article licensed under the Creative Commons Attribution 4.0 International License CC-BY 4.0., which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are properly credited.